Journal of Occupational
Health and Epidemiology

Rafsanjan university Of medical sciences
Volume 12, Issue 4 (Autumn 2023)
J Occup Health Epidemiol 2023, 12(4): 251-259 |
Back to browse issues page



Ethics code: IR.QUMS.REC.1399.374
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tabanfar S, Sobhani S, Safari Variani A, Varmazyar S. The Impact of Strengthening the Neck Muscles on the Pain Prevalence and Neck Disability among Office Workers at Qazvin University of Medical Sciences in 2021, Iran. J Occup Health Epidemiol 2023; 12 (4) :251-259
URL: http://johe.rums.ac.ir/article-1-716-en.html
URL: http://johe.rums.ac.ir/article-1-716-en.html
Related article in
Google Scholar
Google Scholar
Similar articles



1- M.Sc. in Occupational Health Engineering, Faculty of Health, Qazvin University of Medical Science, Qazvin, Iran.
2- Ph.D. Student in Occupational Health Engineering, Dept. of Occupational Health Engineering, School of Public Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
3- Associate Prof. Dept. of Occupational Health Engineering, Faculty of Health, Qazvin University of Medical Sciences, Qazvin, Iran
4- Professor, Dept. of Occupational Health Engineering, Social Determinants of Health Research Center and Research Institute for Prevention of Non-Communicable Diseases, Faculty of Health, Qazvin University of Medical Sciences, Qazvin, Iran. ,svarmazyar@qums.ac.ir
2- Ph.D. Student in Occupational Health Engineering, Dept. of Occupational Health Engineering, School of Public Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
3- Associate Prof. Dept. of Occupational Health Engineering, Faculty of Health, Qazvin University of Medical Sciences, Qazvin, Iran
4- Professor, Dept. of Occupational Health Engineering, Social Determinants of Health Research Center and Research Institute for Prevention of Non-Communicable Diseases, Faculty of Health, Qazvin University of Medical Sciences, Qazvin, Iran. ,
Article history

Received: 2023/03/1
Accepted: 2023/09/30
ePublished: 2023/12/15
Accepted: 2023/09/30
ePublished: 2023/12/15
Subject:
Occupational Health
Keywords: Disability [MeSH], Exercise [MeSH], Neck [MeSH], Office [MeSH], Workers [MeSH], Pain [MeSH]
Full-Text [PDF 497 kb]
(1042 Downloads)
| Abstract (HTML) (2670 Views)
.jpg)
Fig. 1. Disposition of study participants

Table 1. Demographic information of participants in the study
Table 2. The results of the investigation of the neck pain prevalence in office workers and the results of the McNemar test (n=85)
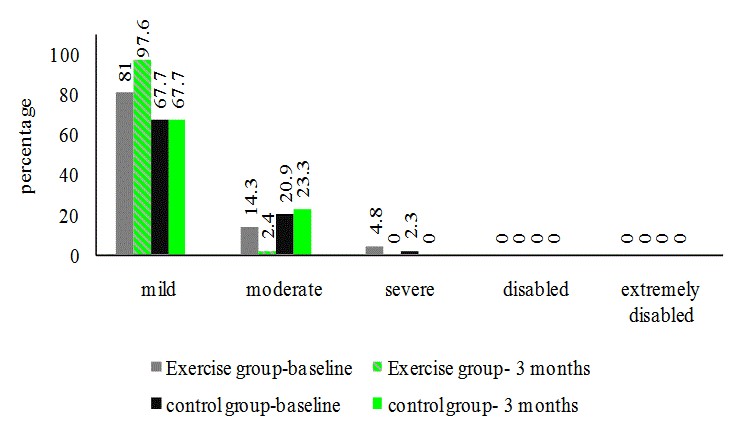
Fig.3.Percentage of neck disability index (qualitative) among office workers
Table 3. Comparing the results of NDI before and after intervention using paired t-test
Discussion
This study investigated the effect of exercise on specific neck muscles in preventing the prevalence of neck pain and neck disability among office workers at the University of Medical Sciences.
In the present study, the neck pain prevalence in office workers during the last 12 months and the last seven days was reported at 47.05% and 40%, respectively. Mohammadipour et al. reported a 12-month prevalence of neck pain of 55.2% in university office workers [12]. In the study of Noroozi et al., the prevalence of neck pain in office workers in the last 12 months and the last seven days was 36% and 25%, respectively [41]. The difference in the prevalence of neck pain in our study could be due to the higher average age and more work participants experience. Based on the results, the neck pain prevalence in the last seven days in the exercise group decreased by 14.29% after the intervention, while there was no change in the prevalence of neck pain in the control group. So, the results showed that exercise can reduce neck pain prevalence among office workers. The data relating to neck pain prevalence in the last seven days showed a statistically significant difference before and after the intervention in the exercise group. Sitthipornvorakul et al. showed that an intervention to increase daily walking steps reduced neck pain prevalence in office workers [7]. Fortún-Rabadán et al.investigated the effectiveness of a multimodal physiotherapy intervention on the improvement of musculoskeletal pain in office workers, and the results showed that the cervical spine was the most common region of pain in the body with 54% and a significant reduction in neck pain intensity observed after the intervention [42].
In a systematic review conducted by Kelly et al., strong evidence was provided to support the effectiveness of physical exercise in controlling neck pain among sedentary staff [43]. Since non-ergonomic equipment is often used in office environments, constant contractions, bending, or rotation of the cervical spine occur abundantly, which can cause discomfort in the neck and shoulders. Studies have shown that in neck trapezius muscles, there is a significant positive relationship between neck bending and skeletal disorders [12]. The study of Anderson et al. reported the beneficial effect of exercise on musculoskeletal pain symptoms in several areas of the upper body, as well as the reduction of the number of pain areas, especially in cases of the neck [44]. Based on the results of this research, it seems that 12 weeks of corrective exercises can reduce neck pain prevalence by strengthening the flexor and scapulothoracic muscles (Rhomboid, middle and lower Trapezius, and Pectoralis). Other possible causes of improvement can include improving the blood circulation system and expanding blood vessels due to performing exercise and relieving muscle fatigue [45]. Therefore, the proposed intervention can be a practical and cost-effective strategy for office work environments to manage neck pain.
In this research, the effects of corrective movements on the neck disability index were evaluated as a pre-test and post-test. Examining the NDI before and after the intervention in the exercise group showed a statistically significant reduction and improvement. The quantitative disability index decreased by 3.24% in the mean number of the index. In the qualitative disability index, the severe category decreased from 4.8% to 0%, and the moderate category decreased from 14.4% to 2%. Also, 97.6% of the exercise group reported a mild disability index after the intervention, but no improvement was observed in the control group. In line with the present study, Imet al. also observed a significant improvement in the neck disability index in the group that performed shoulder stabilization exercises [46]. In the study of Abdel-Aziem et al., which examined the effects of deep flexor exercises on neck pain, performing the exercises after three months showed a significant decrease in the NDI score [17]. In Sarraf et al.'s study with sports intervention similar to the present study on text neck syndrome among university students, the reduction of the neck disability index was matched to our study [40]. Exercises aimed at strengthening the neck and shoulder complex muscles help people to report lower levels of pain and disability during daily activities. Kang et al.investigated the combined effects of scapular stability and chest extension exercises on office workers, and a significant reduction was observed in NDI before and after the intervention in exercise groups. These researchers pointed out that exercise intervention improves the alignment of the cervical spine through proper position, reduces the tension and fatigue of the surface muscles, and, as a result, removes the muscle imbalance. Therefore, pain reduction improves NDI [47]. Lee et al. investigated the effectiveness of implementing McKenzie exercises as a mobile app-based exercise program at the workplace for at least two 10-15-minute sessions in 8 weeks and observed that NDI after the intervention significantly improved [48]. Also, the results of this research determined that performing specific neck muscle strengthening exercises helps to improve the NDI and reduces functional disability, and as a result, improves a person's ability to perform daily activities.
Conclusion
The results of the present study showed that almost half of the office workers participants in this research have suffered from the prevalence of neck pain in the past year. Also, the results of the research confirmed the effect of corrective movements, which included strengthening the flexor, deep neck flexor (Longus Capitis, Longus Colli, and scalene), and scapulothoracic muscles (Rhomboid, Pectoralis, middle and lower Trapezius) in improving the prevalence of neck pain and NDI among office workers. The present study findings can be used to create an exercise program for the musculoskeletal disorders prevention in the neck region among office workers. It is suggested to measure the effect of corrective movements in future studies by examining people through experts and taking nerve and muscle strips at the beginning and end of the intervention. In addition, examining the workstation and people's lifestyles will help to find the cause of neck pain to manage, prevent, correct and improve neck pain.
Acknowledgement
The authors would like to thank office workers at Qazvin University of Medical Sciences for their sincere cooperation in the data collection process.
Conflict of interest: None declared.
Full-Text: (425 Views)
Introduction
Neck pain is a common and often debilitating musculoskeletal disease and it is the fourth cause of disability during years of life for people worldwide [1, 2]. Also, neck pain is one of the most common occupational musculoskeletal disorders, and the job plays a significant role in its development [3]. Neck pain is common among adults and peaks around the age of 45 years [4]. Population studies reported the neck pain prevalence during a person's lifetime to be more than 70% and its point prevalence between 12% and 34% [3, 5]. Chronic neck pain accounts for 14.6% of all musculoskeletal disorders in the general population [6]. Acute neck pain usually improves significantly within two months, but approximately 50% of patients still experience pain or reoccurs within one year after occurrence [4].
Neck pain is the most common musculoskeletal disorder in office environments [7]. Office workers are exposed to muscle tension and suffer from musculoskeletal disorders, especially neck pain, due to maintaining a static position for a long time, working with computers, using non-ergonomic equipment, repetitive tasks, high workload, and lack of breaks [3, 8-10]. A cross-sectional study estimated the one-year prevalence of neck pain among office workers at 45.5% [11]. In the study conducted among university office workers in Iran, neck pain was reported as 55.2% [12]. Also, Sohrabi et al. estimated the highest prevalence of musculoskeletal disorders in Iranian employees in 2022 in the neck region at 57% [13]. Nunes et al. reported the prevalence of neck pain in Portuguese office workers as 56.1% [14]. Office workers are 2-3 times more likely to suffer from neck pain than the general population, and the most common cause of absenteeism among these people is pain or sensitivity in the neck region [15]. Identifying neck pain risk factors and their consequences can help prevent, diagnose, treat, and manage [10].
One of the main strategies for managing neck pain is exercise therapy [16]. Exercise therapy includes strength, stabilization, and endurance exercises that are defined as a physical activity program that is designed and prescribed for therapeutic purposes [1] People with neck pain when they are distracted, put their head forward and experience abnormal movement control of the deep neck flexors and fatigue under voluntary contraction, which leads to fatigue in the neck muscles [4]. As a result, neck pain affects superficial muscle strength, deep neck flexor endurance, and muscle performance capacity [4, 17].
A recent systematic review of patients with neck pain showed that multimodal exercises (exercises affecting deep and superficial neck muscles) with beneficial effects on neck function and symptom control are essential [6]. The underlying mechanisms of neck pain prevention, recurrence, and progression are unclear. Still, they may be related to strengthening neck muscles, which play a decisive role in neck joint position and head movement control [18]. When the scapulothoracic muscles are disturbed, the upper trapezius tightens, the middle and lower trapezius weak, and muscle imbalance occurs in the scapular region. Exercises that increase the strength of the lower trapezius to the upper trapezius ratio suggest a pain decrease [19]. Also, several studies have shown the relationship between the decreased strength and endurance of the neck's deep and anterior flexor muscles and neck pain [17, 20, 21].
On the other hand, exercises that affect the neck's deep flexor muscles reduce the symptoms of neck pain,increase its activation, and may improve the ability to maintain the vertical position of the cervical spine [17]. However, Griffiths et al. stated that there is no clear benefit of including specific neck exercises in chronic neck pain treatment in general [22]. Gross et al. also stated that there is uncertainty regarding the effectiveness of exercise for neck pain [23].
Despite the various studies conducted about the effects of exercise in improving neck pain, the evidence regarding exercise therapy for neck pain is still limited and controversial [24]. Since office workers comprise a large part of the workforce and the effort to maintain the health of these people is considered an important issue, this study aimed to investigate the impact of exercise intervention by strengthening the neck muscles on the pain prevalence and neck disability among office workers.
Materials and Methods
The present research was an interventional study conducted during March, April, and May 2021 among 85 subjects (50 female and 35 male) of the office workers at Qazvin University of Medical Sciences. All participants entered the study after completing the consent form.
Participants who completed the inclusion criteria were randomly assigned to the exercise or control groups using computer-generated random numbers. Randomization was performed by a researcher independent of the study. Allocation was done according to the principle of similarity in the groups. One of the researchers collected the data related to the pre-intervention, and another evaluated the results so that he was unaware of the allocation groups.
The participants were office workers who generally performed their duties as sitting during an 8-hour shift and worked with computers (monitor, keyboard, and mouse), telephone, and documents. Consequently, the computer workstation strongly affects neck pain.
According to the mean and standard deviation of neck pain in previous studies [25] and using equation 1 (α=0.05, β=0.1, S1=1.37, S2=1.82, μ1=1.89, μ2=3.32, Z1-α/2=1.96, and Z1-β=1.28) the number of samples of each group (control and exercise) was estimated to be 27 people.
Formula 1.
.jpg)
α: Error probability of type I
β: Error probability Type II
S1: standard deviation in the first group (Exercise group)
S2: standard deviation in the second group (control group)
μ1: Mean in the first group (Exercise group)
μ2: Mean in the second group (control group)
The process of selecting the sample is shown in Figure 1. Given the willingness of subjects finally, 85 subjects (exercise group=42 subjects, control group=43 subjects) participated in the study.
Inclusion criteria were having at least one year of history with computers [7], a body mass index 25 kg/m2, and suffering from mild and higher neck pain intensity. Exclusion criteria were leaving the workplace more than one month due to illness during the last year, having developmental and congenital diseases in the head and neck, inflammatory diseases in the neck, neuromuscular disorders in the neck, a history of head
and neck surgery, problems in the cervical vertebrae, and any uncorrected vision or hearing problems, unwilling to participate in the exercises, performing sports activities simultaneously with the corrective exercises, experiencing an accident and injury in the neck for various reasons during the research, and absenteeism in corrective exercises for > 2 weeks [8, 26-31].
Neck pain is a common and often debilitating musculoskeletal disease and it is the fourth cause of disability during years of life for people worldwide [1, 2]. Also, neck pain is one of the most common occupational musculoskeletal disorders, and the job plays a significant role in its development [3]. Neck pain is common among adults and peaks around the age of 45 years [4]. Population studies reported the neck pain prevalence during a person's lifetime to be more than 70% and its point prevalence between 12% and 34% [3, 5]. Chronic neck pain accounts for 14.6% of all musculoskeletal disorders in the general population [6]. Acute neck pain usually improves significantly within two months, but approximately 50% of patients still experience pain or reoccurs within one year after occurrence [4].
Neck pain is the most common musculoskeletal disorder in office environments [7]. Office workers are exposed to muscle tension and suffer from musculoskeletal disorders, especially neck pain, due to maintaining a static position for a long time, working with computers, using non-ergonomic equipment, repetitive tasks, high workload, and lack of breaks [3, 8-10]. A cross-sectional study estimated the one-year prevalence of neck pain among office workers at 45.5% [11]. In the study conducted among university office workers in Iran, neck pain was reported as 55.2% [12]. Also, Sohrabi et al. estimated the highest prevalence of musculoskeletal disorders in Iranian employees in 2022 in the neck region at 57% [13]. Nunes et al. reported the prevalence of neck pain in Portuguese office workers as 56.1% [14]. Office workers are 2-3 times more likely to suffer from neck pain than the general population, and the most common cause of absenteeism among these people is pain or sensitivity in the neck region [15]. Identifying neck pain risk factors and their consequences can help prevent, diagnose, treat, and manage [10].
One of the main strategies for managing neck pain is exercise therapy [16]. Exercise therapy includes strength, stabilization, and endurance exercises that are defined as a physical activity program that is designed and prescribed for therapeutic purposes [1] People with neck pain when they are distracted, put their head forward and experience abnormal movement control of the deep neck flexors and fatigue under voluntary contraction, which leads to fatigue in the neck muscles [4]. As a result, neck pain affects superficial muscle strength, deep neck flexor endurance, and muscle performance capacity [4, 17].
A recent systematic review of patients with neck pain showed that multimodal exercises (exercises affecting deep and superficial neck muscles) with beneficial effects on neck function and symptom control are essential [6]. The underlying mechanisms of neck pain prevention, recurrence, and progression are unclear. Still, they may be related to strengthening neck muscles, which play a decisive role in neck joint position and head movement control [18]. When the scapulothoracic muscles are disturbed, the upper trapezius tightens, the middle and lower trapezius weak, and muscle imbalance occurs in the scapular region. Exercises that increase the strength of the lower trapezius to the upper trapezius ratio suggest a pain decrease [19]. Also, several studies have shown the relationship between the decreased strength and endurance of the neck's deep and anterior flexor muscles and neck pain [17, 20, 21].
On the other hand, exercises that affect the neck's deep flexor muscles reduce the symptoms of neck pain,increase its activation, and may improve the ability to maintain the vertical position of the cervical spine [17]. However, Griffiths et al. stated that there is no clear benefit of including specific neck exercises in chronic neck pain treatment in general [22]. Gross et al. also stated that there is uncertainty regarding the effectiveness of exercise for neck pain [23].
Despite the various studies conducted about the effects of exercise in improving neck pain, the evidence regarding exercise therapy for neck pain is still limited and controversial [24]. Since office workers comprise a large part of the workforce and the effort to maintain the health of these people is considered an important issue, this study aimed to investigate the impact of exercise intervention by strengthening the neck muscles on the pain prevalence and neck disability among office workers.
Materials and Methods
The present research was an interventional study conducted during March, April, and May 2021 among 85 subjects (50 female and 35 male) of the office workers at Qazvin University of Medical Sciences. All participants entered the study after completing the consent form.
Participants who completed the inclusion criteria were randomly assigned to the exercise or control groups using computer-generated random numbers. Randomization was performed by a researcher independent of the study. Allocation was done according to the principle of similarity in the groups. One of the researchers collected the data related to the pre-intervention, and another evaluated the results so that he was unaware of the allocation groups.
The participants were office workers who generally performed their duties as sitting during an 8-hour shift and worked with computers (monitor, keyboard, and mouse), telephone, and documents. Consequently, the computer workstation strongly affects neck pain.
According to the mean and standard deviation of neck pain in previous studies [25] and using equation 1 (α=0.05, β=0.1, S1=1.37, S2=1.82, μ1=1.89, μ2=3.32, Z1-α/2=1.96, and Z1-β=1.28) the number of samples of each group (control and exercise) was estimated to be 27 people.
Formula 1.
α: Error probability of type I
β: Error probability Type II
S1: standard deviation in the first group (Exercise group)
S2: standard deviation in the second group (control group)
μ1: Mean in the first group (Exercise group)
μ2: Mean in the second group (control group)
The process of selecting the sample is shown in Figure 1. Given the willingness of subjects finally, 85 subjects (exercise group=42 subjects, control group=43 subjects) participated in the study.
Inclusion criteria were having at least one year of history with computers [7], a body mass index 25 kg/m2, and suffering from mild and higher neck pain intensity. Exclusion criteria were leaving the workplace more than one month due to illness during the last year, having developmental and congenital diseases in the head and neck, inflammatory diseases in the neck, neuromuscular disorders in the neck, a history of head
and neck surgery, problems in the cervical vertebrae, and any uncorrected vision or hearing problems, unwilling to participate in the exercises, performing sports activities simultaneously with the corrective exercises, experiencing an accident and injury in the neck for various reasons during the research, and absenteeism in corrective exercises for > 2 weeks [8, 26-31].
Fig. 1. Disposition of study participants
Nordic Musculoskeletal Questionnaire (NMQ): The sections related to neck discomfort of the Nordic Musculoskeletal Questionnaire (NMQ) provided by the National Institute of Occupational Safety and Health (NIOSH) were used to detect neck pain prevalence. This questionnaire examines neck pain, discomfort, and burning during the last 12 months and the seven days (32). This tool is widely used in occupational research and is a valid and reliable tool. The validity of the Persian version of this questionnaire was confirmed by Choobineh et al. (33, 34). The present study used 7 days and 12 months to investigate acute and chronic neck pain, respectively.
Neck Disability Index Questionnaire (NDI): Neck Disability Index was used to investigate the self-reported functional disability of neck pain, which shows the effect of neck pain on a person's ability to perform daily activities. This questionnaire includes ten questions about pain intensity, reading, lifting objects, personal work, study, headache, concentration, recreation, driving, and work. Each question contains six options (0: no pain to 5: worst imaginable pain). The total score is a number between 0 and 50 (18). The disability of each person is shown as a percentage from 0% (no problem) to 100% (completely disabled). The severity of the disability is 0-20% mild, 21-40% moderate, 41-60% severe, 61-80% disabled, and 81-100% extremely disabled (35). The NDI questionnaire has high reliability and validity with intragroup correlation (ICC) of 0.88 to 0.95 and high internal consistency with Cronbach's α from 0.85 to 0.90 (36). The NDI is a valid tool with pre-test-post-test reliability used for self-reporting neck pain among office workers (37).
Exercise Intervention: Exercises were designed by a specialist in corrective movements and sports medicine after the approval of two experts in this field and based on the exercises presented in valid previous research and articles (Figure 2) (38). The sport protocol design directly affected the target muscles and included flexors, deep flexors, and scapulothoracic (rhomboid, pectoralis, middle, and lower trapezius). A review by O'Riordan et al. recommended that effective interventions must last between 6 and 12 weeks (39). Sarraf et al. showed the effect of sports intervention on neck pain for eight weeks, five times per week, and once a day (40). Therefore, according to the studies and experts' opinion. The intervention was done for 12 weeks (three months), five sessions per week, and each session 15 minutes in the exercise group, and no intervention was done in the control group. At first, the sports group was trained on the correct way to perform sports movements and received a training file, a video on how to do the exercises. Also, they received the basic principles and tips for doing the activities along with the tables for recording the days and performing times per week. The sports movements were designed in a way that could be done at work and home.
Neck Disability Index Questionnaire (NDI): Neck Disability Index was used to investigate the self-reported functional disability of neck pain, which shows the effect of neck pain on a person's ability to perform daily activities. This questionnaire includes ten questions about pain intensity, reading, lifting objects, personal work, study, headache, concentration, recreation, driving, and work. Each question contains six options (0: no pain to 5: worst imaginable pain). The total score is a number between 0 and 50 (18). The disability of each person is shown as a percentage from 0% (no problem) to 100% (completely disabled). The severity of the disability is 0-20% mild, 21-40% moderate, 41-60% severe, 61-80% disabled, and 81-100% extremely disabled (35). The NDI questionnaire has high reliability and validity with intragroup correlation (ICC) of 0.88 to 0.95 and high internal consistency with Cronbach's α from 0.85 to 0.90 (36). The NDI is a valid tool with pre-test-post-test reliability used for self-reporting neck pain among office workers (37).
Exercise Intervention: Exercises were designed by a specialist in corrective movements and sports medicine after the approval of two experts in this field and based on the exercises presented in valid previous research and articles (Figure 2) (38). The sport protocol design directly affected the target muscles and included flexors, deep flexors, and scapulothoracic (rhomboid, pectoralis, middle, and lower trapezius). A review by O'Riordan et al. recommended that effective interventions must last between 6 and 12 weeks (39). Sarraf et al. showed the effect of sports intervention on neck pain for eight weeks, five times per week, and once a day (40). Therefore, according to the studies and experts' opinion. The intervention was done for 12 weeks (three months), five sessions per week, and each session 15 minutes in the exercise group, and no intervention was done in the control group. At first, the sports group was trained on the correct way to perform sports movements and received a training file, a video on how to do the exercises. Also, they received the basic principles and tips for doing the activities along with the tables for recording the days and performing times per week. The sports movements were designed in a way that could be done at work and home.
Fig. 2. Exercises used in the sports intervention and the muscles involved
Description of how to do exercises provided following up:
Number 1: Bringing the chin closer to the neck and holding it (3 sets, each set 10 times and rest 10 seconds between sets).
Number 2: Keep the chin close to the neck and apply pressure from the forehead to the hands (3 sets, each set 15 times and rest 15 seconds between sets).
Number 3: Connecting the arms to the body by bending the elbows, converging and contracting the shoulders and keeping both shoulders in a "W" shape, and stretching both arms in a "V" shape (3 sets, each set 10 times and rest 10 seconds between sets).
Number 4: Connecting the arms to the body, bending the elbows 90 degrees with the body, and convergence and contraction of both shoulders and pulling out the elastic band (3 sets, each set 10 times and rest 10 seconds between sets).
Number 5: Connecting the arms to the body by bending the elbows and converging and contracting both shoulders (3 sets, each set 10 times and rest 10 seconds between sets).
Number 6: Stretching the arms, bending the elbows 90 degrees with the plane, and converging and contracting both shoulders (3 sets, each set 10 times and rest 10 seconds between sets).
Number 7: Tilting the neck to the left side so that the right side of the neck muscle is stretched, holding the right hand to the chair, and applying pressure to the head through the left hand - oppositely performing the exercise for the right side (3 sets, each set 10 times and rest 10 seconds between sets).
Number 8: Tilting the head to the left so that the posterior neck muscle is stretched, holding the right hand to the chair, and applying pressure on the head through the left hand (3 sets, each set 10 times and rest 10 or 20 seconds between sets).
Number 9: Stretching the shoulder height towards the wall, then reaching it forward, feeling the pressure on the chest, and holding it (3 sets, each set 10 times and rest 10 seconds between sets).
Number 10: Sitting on a chair, connecting the back to the backrest, closing the hands behind the neck with the elbows extended and the back supported (3 sets, each set 10 times and rest 20 seconds between sets).
The data was analyzed using SPSS version 26 software. Descriptive statistics of demographic information and investigated variables among participants were presented in frequency, percentage, mean, and standard deviation. The Kolmogorov-Smirnov test was used for the data normality distribution. To check the prevalence of neck pain before and after the intervention, the McNemar test and the NDI were used using the paired t-test. Statistical analysis was considered at a 95% confidence level and P < 0.05.
It should be noted that this article is taken from the thesis approved by the Research Assistant of Qazvin
University of Medical Sciences under IR.QUMS.REC.1399.374.
Results
The mean and standard deviation of the age of both the exercise and control groups were 41.74 ± 7.55 and 42.53 ± 8.04 years, respectively (Table 1).To check the similarity between the exercise and control groups, variables age, height, weight, body mass index, and work history were examined. The results showed that the two group’s statistically significant differences did not.
Number 1: Bringing the chin closer to the neck and holding it (3 sets, each set 10 times and rest 10 seconds between sets).
Number 2: Keep the chin close to the neck and apply pressure from the forehead to the hands (3 sets, each set 15 times and rest 15 seconds between sets).
Number 3: Connecting the arms to the body by bending the elbows, converging and contracting the shoulders and keeping both shoulders in a "W" shape, and stretching both arms in a "V" shape (3 sets, each set 10 times and rest 10 seconds between sets).
Number 4: Connecting the arms to the body, bending the elbows 90 degrees with the body, and convergence and contraction of both shoulders and pulling out the elastic band (3 sets, each set 10 times and rest 10 seconds between sets).
Number 5: Connecting the arms to the body by bending the elbows and converging and contracting both shoulders (3 sets, each set 10 times and rest 10 seconds between sets).
Number 6: Stretching the arms, bending the elbows 90 degrees with the plane, and converging and contracting both shoulders (3 sets, each set 10 times and rest 10 seconds between sets).
Number 7: Tilting the neck to the left side so that the right side of the neck muscle is stretched, holding the right hand to the chair, and applying pressure to the head through the left hand - oppositely performing the exercise for the right side (3 sets, each set 10 times and rest 10 seconds between sets).
Number 8: Tilting the head to the left so that the posterior neck muscle is stretched, holding the right hand to the chair, and applying pressure on the head through the left hand (3 sets, each set 10 times and rest 10 or 20 seconds between sets).
Number 9: Stretching the shoulder height towards the wall, then reaching it forward, feeling the pressure on the chest, and holding it (3 sets, each set 10 times and rest 10 seconds between sets).
Number 10: Sitting on a chair, connecting the back to the backrest, closing the hands behind the neck with the elbows extended and the back supported (3 sets, each set 10 times and rest 20 seconds between sets).
The data was analyzed using SPSS version 26 software. Descriptive statistics of demographic information and investigated variables among participants were presented in frequency, percentage, mean, and standard deviation. The Kolmogorov-Smirnov test was used for the data normality distribution. To check the prevalence of neck pain before and after the intervention, the McNemar test and the NDI were used using the paired t-test. Statistical analysis was considered at a 95% confidence level and P < 0.05.
It should be noted that this article is taken from the thesis approved by the Research Assistant of Qazvin
University of Medical Sciences under IR.QUMS.REC.1399.374.
Results
The mean and standard deviation of the age of both the exercise and control groups were 41.74 ± 7.55 and 42.53 ± 8.04 years, respectively (Table 1).To check the similarity between the exercise and control groups, variables age, height, weight, body mass index, and work history were examined. The results showed that the two group’s statistically significant differences did not.
Table 1. Demographic information of participants in the study
| Quantitative information | Qualitative information | ||||||
| Variable | Mean± SD | P-value | Variable | Category | Number (%) | ||
| Experimental group (n=42) | Control group (n=43) | Experimental group (n=42) | Control group (n=43) | ||||
| Height(cm) | 166.33±9.38 | 168.49±7.99 | 0.294 | Gender | Male | 17 (40.5) | 18 (41.9) |
| Weight(kg) | 65.94±8 | 66±8.17 | 0.948 | Female | 25 (59.5) | 25 (58.1) | |
| BMI(kg/m2) | 23.76±1.27 | 23.16±1.46 | 0.174 | Marital Status | Single | 6 (14.3) | 9(20.9) |
| Work Experience (y) | 16.36±6.76 | 16.07±6.95 | 0.691 | Married | 36 (85.7) | 34(79.1) | |
The prevalence of neck pain in participants in the last 12 months and seven days was 47.05% and 40%, respectively (Table 2). Neck pain in the last seven days decreased by 14.29% in the exercise group after the intervention. Considering that the intervention was implemented overthree months, for assessing the effectiveness of the exercise program, the neck region pain related to the last seven days was re-examined after the end of the intervention. The prevalence of neck pain in the last seven days using the McNemar test showed a statistically significant difference (P=0.031) before and after the intervention of corrective exercises in the exercise group (Table 2).
Table 2. The results of the investigation of the neck pain prevalence in office workers and the results of the McNemar test (n=85)
| Variable | All participants(n=85) n (%) |
Exercise group n (%) |
P-value | Control group n (%) |
P-value | ||
| Baseline | 3 months | Baseline | 3 months | ||||
| Pain, discomfort, burning, or numbness in the neck area in the last 7 days | 34(40.00) | 14(33.33) | 8(19.04) | 0.031 | 20(46.51) | 24(55.81) | 0.375 |
| Pain, discomfort, burning, or numbness in the neck area in the last 12 months | 40(47.05) | 21(50.00) | - | - | 19(44.18) | - | - |
| Resting, reducing work activity, leaving the workplace, or being unable to perform activities at work or at home due to pain or discomfort in the neck region in the last 12 months | 16(18.82) | 9(21.42) | - | - | 7(16.27) | - | - |
| See a doctor because of neck pains | 11(12.94) | 10(23.8) | - | - | 1(2.32) | - | - |
According to the frequency distribution of NDI (Fig. 3), the severe category decreased from 4.8% to 0%, and the moderate category decreased from 14.3% to 2.4% in the exercise group after the intervention. Comparing the NDI (Table 3) before and after the intervention showed a significant decrease in the exercise group (p=0.007), while no significant difference was found in the control group (p=0.58).
Fig.3.Percentage of neck disability index (qualitative) among office workers
Table 3. Comparing the results of NDI before and after intervention using paired t-test
| Variable | group | Time | Mean | SD | t | P-value |
| NDI | Exercise group | Baseline | 6.64 | 5.89 | 6.86 | 0.007 |
| 3 months | 3.40 | 3.30 | ||||
| control group | Baseline | 6.35 | 6.14 | -0.55 | 0.58 | |
| 3 months | 6.77 | 5.67 |
Discussion
This study investigated the effect of exercise on specific neck muscles in preventing the prevalence of neck pain and neck disability among office workers at the University of Medical Sciences.
In the present study, the neck pain prevalence in office workers during the last 12 months and the last seven days was reported at 47.05% and 40%, respectively. Mohammadipour et al. reported a 12-month prevalence of neck pain of 55.2% in university office workers [12]. In the study of Noroozi et al., the prevalence of neck pain in office workers in the last 12 months and the last seven days was 36% and 25%, respectively [41]. The difference in the prevalence of neck pain in our study could be due to the higher average age and more work participants experience. Based on the results, the neck pain prevalence in the last seven days in the exercise group decreased by 14.29% after the intervention, while there was no change in the prevalence of neck pain in the control group. So, the results showed that exercise can reduce neck pain prevalence among office workers. The data relating to neck pain prevalence in the last seven days showed a statistically significant difference before and after the intervention in the exercise group. Sitthipornvorakul et al. showed that an intervention to increase daily walking steps reduced neck pain prevalence in office workers [7]. Fortún-Rabadán et al.investigated the effectiveness of a multimodal physiotherapy intervention on the improvement of musculoskeletal pain in office workers, and the results showed that the cervical spine was the most common region of pain in the body with 54% and a significant reduction in neck pain intensity observed after the intervention [42].
In a systematic review conducted by Kelly et al., strong evidence was provided to support the effectiveness of physical exercise in controlling neck pain among sedentary staff [43]. Since non-ergonomic equipment is often used in office environments, constant contractions, bending, or rotation of the cervical spine occur abundantly, which can cause discomfort in the neck and shoulders. Studies have shown that in neck trapezius muscles, there is a significant positive relationship between neck bending and skeletal disorders [12]. The study of Anderson et al. reported the beneficial effect of exercise on musculoskeletal pain symptoms in several areas of the upper body, as well as the reduction of the number of pain areas, especially in cases of the neck [44]. Based on the results of this research, it seems that 12 weeks of corrective exercises can reduce neck pain prevalence by strengthening the flexor and scapulothoracic muscles (Rhomboid, middle and lower Trapezius, and Pectoralis). Other possible causes of improvement can include improving the blood circulation system and expanding blood vessels due to performing exercise and relieving muscle fatigue [45]. Therefore, the proposed intervention can be a practical and cost-effective strategy for office work environments to manage neck pain.
In this research, the effects of corrective movements on the neck disability index were evaluated as a pre-test and post-test. Examining the NDI before and after the intervention in the exercise group showed a statistically significant reduction and improvement. The quantitative disability index decreased by 3.24% in the mean number of the index. In the qualitative disability index, the severe category decreased from 4.8% to 0%, and the moderate category decreased from 14.4% to 2%. Also, 97.6% of the exercise group reported a mild disability index after the intervention, but no improvement was observed in the control group. In line with the present study, Imet al. also observed a significant improvement in the neck disability index in the group that performed shoulder stabilization exercises [46]. In the study of Abdel-Aziem et al., which examined the effects of deep flexor exercises on neck pain, performing the exercises after three months showed a significant decrease in the NDI score [17]. In Sarraf et al.'s study with sports intervention similar to the present study on text neck syndrome among university students, the reduction of the neck disability index was matched to our study [40]. Exercises aimed at strengthening the neck and shoulder complex muscles help people to report lower levels of pain and disability during daily activities. Kang et al.investigated the combined effects of scapular stability and chest extension exercises on office workers, and a significant reduction was observed in NDI before and after the intervention in exercise groups. These researchers pointed out that exercise intervention improves the alignment of the cervical spine through proper position, reduces the tension and fatigue of the surface muscles, and, as a result, removes the muscle imbalance. Therefore, pain reduction improves NDI [47]. Lee et al. investigated the effectiveness of implementing McKenzie exercises as a mobile app-based exercise program at the workplace for at least two 10-15-minute sessions in 8 weeks and observed that NDI after the intervention significantly improved [48]. Also, the results of this research determined that performing specific neck muscle strengthening exercises helps to improve the NDI and reduces functional disability, and as a result, improves a person's ability to perform daily activities.
Conclusion
The results of the present study showed that almost half of the office workers participants in this research have suffered from the prevalence of neck pain in the past year. Also, the results of the research confirmed the effect of corrective movements, which included strengthening the flexor, deep neck flexor (Longus Capitis, Longus Colli, and scalene), and scapulothoracic muscles (Rhomboid, Pectoralis, middle and lower Trapezius) in improving the prevalence of neck pain and NDI among office workers. The present study findings can be used to create an exercise program for the musculoskeletal disorders prevention in the neck region among office workers. It is suggested to measure the effect of corrective movements in future studies by examining people through experts and taking nerve and muscle strips at the beginning and end of the intervention. In addition, examining the workstation and people's lifestyles will help to find the cause of neck pain to manage, prevent, correct and improve neck pain.
Acknowledgement
The authors would like to thank office workers at Qazvin University of Medical Sciences for their sincere cooperation in the data collection process.
Conflict of interest: None declared.
References
1. Fredin K, Lorås H. Manual therapy, exercise therapy or combined treatment in the management of adult neck pain–a systematic review and meta-analysis. Musculoskelet Sci Pract. 2017;31:62-71. [DOI] [PMID]
2. Alshami AM, AlSadiq AI. Outcomes of scapulothoracic mobilisation in patients with neck pain and scapular dyskinesis: A randomised clinical trial. J Taibah Univ Med Sci. 2021;16(4):540-9. [DOI] [PMID] [PMCID]
3. Iqbal ZA, Alghadir AH, Anwer S. Efficacy of deep cervical flexor muscle training on neck pain, functional disability, and muscle endurance in school teachers: a clinical trial. Biomed Res Int. 2021;2021:7190808 [DOI] [PMID] [PMCID]
4. Lin IH, Chang KH, Liou TH, Tsou CM, Huang YC. Progressive shoulder-neck exercise on cervical muscle functions in middle-aged and senior patients with chronic neck pain. Eur J Phys Rehabil Med. 2018;54(1):13-21. [DOI] [PMID]
5. Cagnie B, Danneels L, Van Tiggelen D, De Loose V, Cambier D. Individual and work related risk factors for neck pain among office workers: a cross sectional study. Eur Spine J. 2007;16(5):679-86. [DOI] [PMID] [PMCID]
6. Rodríguez-Sanz J, Malo-Urriés M, Corral-de-Toro J, López-de-Celis C, Lucha-López MO, Tricás-Moreno JM, et al. Does the addition of manual therapy approach to a cervical exercise program improve clinical outcomes for patients with chronic neck pain in short-and mid-term? A randomized controlled trial. Int J Environ Res Public Health. 2020;17(18):6601. [DOI] [PMID] [PMCID]
7. Sitthipornvorakul E, Sihawong R, Waongenngarm P, Janwantanakul P. The effects of walking intervention on preventing neck pain in office workers: a randomized controlled trial. J Occup Health. 2020;62(1):e12106. [DOI] [PMID] [PMCID]
8. Tunwattanapong P, Kongkasuwan R, Kuptniratsaikul V. The effectiveness of a neck and shoulder stretching exercise program among office workers with neck pain: a randomized controlled trial. Clin Rehabil. 2016;30(1):64-72. [DOI] [PMID]
9. da Silva NC, Ricci FPFM, de Castro VR, de Lima ACR, do Carmo Lopes ER, de Salvo Mauad LD, et al. Effects of workplace upper extremity resistance exercises on function and symptoms of workers at a tertiary hospital: a randomized controlled trial protocol. BMC Musculoskelet Disord. 2022;23(1):119. [DOI] [PMID] [PMCID]
10. Kazeminasab S, Nejadghaderi SA, Amiri P, Pourfathi H, Araj-Khodaei M, Sullman MJM, et al. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022;23(1):26. [DOI] [PMID] [PMCID]
11. Markopoulos P, Shen X, Wang Q, Timmermans A. Neckio: Motivating neck exercises in computer workers. Sensors (Basel). 2020;20(17):4928. [DOI] [PMID] [PMCID]
12. Mohammadipour F, Pourranjbar M, Naderi S, Rafie F. Work-related Musculoskeletal Disorders in Iranian Office Workers: Prevalence and Risk Factors. J Med Life. 2018;11(4):328-33. [DOI] [PMID] [PMCID]
13. Sohrabi MS, Babamiri M. Effectiveness of an ergonomics training program on musculoskeletal disorders, job stress, quality of work-life and productivity in office workers: a quasi-randomized control trial study. Int J Occup Saf Ergon. 2022;28(3):1664-71. [DOI] [PMID]
14. Nunes A, Espanha M, Teles J, Petersen K, Arendt-Nielsen L, Carnide F. Neck pain prevalence and associated occupational factors in Portuguese office workers. Int J Ind Ergon. 2021;85:103172. [DOI]
15. Louw S, Makwela S, Manas L, Meyer L, Terblanche D, Brink Y. Effectiveness of exercise in office workers with neck pain: A systematic review and meta-analysis. S Afr J Physiother. 2017;73(1):392. [DOI] [PMID] [PMCID]
16. Tabanfar S, Safari Variani A, Sobhani S, Varmazyar S. The Effect of Self-management Exercises on Neck Pain and Head and Neck Angles among Iranian University Employees: An Interventional Study. Journal of Occupational Health and Epidemiology. 2022;11(2):138-47 [DOI]
17. Abdel-Aziem AA, Draz AH. Efficacy of deep neck flexor exercise for neck pain: A randomized controlled study. Turk J Phys Med Rehabil. 2016;62(2):107-15. [DOI]
18. Bernal-Utrera C, Gonzalez-Gerez JJ, Anarte-Lazo E, Rodriguez-Blanco C. Manual therapy versus therapeutic exercise in non-specific chronic neck pain: a randomized controlled trial. Trials. 2020;21(1):682. [DOI] [PMID] [PMCID]
19. Petersen SM, Wyatt SN. Lower trapezius muscle strength in individuals with unilateral neck pain. J Orthop Sports Phys Ther. 2011;41(4):260-5. [DOI] [PMID]
20. Karaağaç A, Arslan SA, Keskin ED. Assessment of pain, scapulothoracic muscle strength, endurance and scapular dyskinesis in individuals with and without nonspecific chronic neck pain: A cross-sectional study. J Bodyw Mov Ther. 2023;35:261-7. [DOI] [PMID]
21. Dere T, Alemdaroğlu-Gürbüz İ. Muscular endurance and its association with neck pain, disability, neck awareness, and kinesiophobia in patients with chronic neck pain. Somatosens Mot Res. 2023:1-8. [DOI] [PMID]
22. Griffiths C, Dziedzic K, Waterfield J, Sim J. Effectiveness of specific neck stabilization exercises or a general neck exercise program for chronic neck disorders: a randomized controlled trial. J Rheumatol. 2009;36(2):390-7. [DOI] [PMID]
23. Gross A, Kay TM, Paquin JP, Blanchette S, Lalonde P, Christie T, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2015(1):CD004250. [DOI] [PMID] [PMCID]
24. Seo J, Song C, Shin D. A Single-Center Study Comparing the Effects of Thoracic Spine Manipulation vs Mobility Exercises in 26 Office Workers with Chronic Neck Pain: A Randomized Controlled Clinical Study. Med Sci Monit. 2022;28:e937316. [DOI] [PMID] [PMCID]
25. Daher A, Carel RS, Tzipi K, Esther H, Dar G. The effectiveness of an aerobic exercise training on patients with neck pain during a short- and long-term follow-up: a prospective double-blind randomized controlled trial. Clin Rehabil. 2020;34(5):617-29. [DOI] [PMID]
26. Welch A, Healy G, Straker L, Comans T, O’Leary S, Melloh M, et al. Process evaluation of a workplace-based health promotion and exercise cluster-randomised trial to increase productivity and reduce neck pain in office workers: a RE-AIM approach. BMC Public Health. 2020;20(1):180. [DOI] [PMID] [PMCID]
27. Ting JZR, Chen X, Johnston V. Workplace-based exercise intervention improves work ability in office workers: a cluster randomised controlled trial. Int J Environ Res Public Health. 2019;16(15):2633. [DOI] [PMID] [PMCID]
28. Shariat A, Cleland JA, Danaee M, Kargarfard M, Sangelaji B, Tamrin SBM. Effects of stretching exercise training and ergonomic modifications on musculoskeletal discomforts of office workers: a randomized controlled trial. Braz J Phys Ther. 2018;22(2):144-53. [DOI] [PMID] [PMCID]
29. Tejera DM, Beltran-Alacreu H, Cano-de-la-Cuerda R, Leon Hernández JV, Martín-Pintado-Zugasti A, Calvo-Lobo C, et al. Effects of virtual reality versus exercise on pain, functional, somatosensory and psychosocial outcomes in patients with non-specific chronic neck pain: A randomized clinical trial. Int J Environ Res Public Health. 2020;17(16):5950. [DOI] [PMID] [PMCID]
30. Villanueva A, Rabal-Pelay J, Berzosa C, Gutiérrez H, Cimarras-Otal C, Lacarcel-Tejero B, et al. Effect of a Long Exercise Program in the Reduction of Musculoskeletal Discomfort in Office Workers. Int J Environ Res Public Health. 2020;17(23):9042. [DOI] [PMID] [PMCID]
31. Sarraf F, Varmazyar S. Comparing the effect of the posture of using smartphones on head and neck angles among college students. Ergonomics. 2022;65(12):1631-8. [DOI] [PMID]
32. Rahimi F, Kazemi K, Zahednejad S, López-López D, Calvo-Lobo C. Prevalence of work-related musculoskeletal disorders in Iranian physical therapists: a cross-sectional study. J Manipulative Physiol Ther. 2018;41(6):503-7. [DOI] [PMID]
33. Veisi H, Choobineh AR, Ghaem H. Musculoskeletal problems in Iranian hand-woven shoe-sole making operation and developing guidelines for workstation design. Int J Occup Environ Med. 2016;7(2):87-97. [DOI] [PMID] [PMCID]
34. Choobineh A, Lahmi M, Shahnavaz H, Khani Jazani RK, Hosseini M. Musculoskeletal symptoms as related to ergonomic factors in Iranian hand-woven carpet industry and general guidelines for workstation design. Int J Occup Saf Ergon. 2004;10(2):157-68. [DOI] [PMID]
35. Eftekhar Sadat B, Babaei-Ghazani A, Azizi R, Parizad M. Prevalence and risk factors of neck and shoulder pain in medical students of Tabriz University of Medical Sciences. Med J Tabriz Univ Med Sci. 2013;35(3):12-7 [Article]
36. Alfawaz S, Lohman E, Alameri M, Daher N, Jaber H. Effect of adding stretching to standardized procedures on cervical range of motion, pain, and disability in patients with non-specific mechanical neck pain: A randomized clinical trial. J Bodyw Mov Ther. 2020;24(3):50-8. [DOI] [PMID]
37. Kaya Aytutuldu G, Birinci T, Tarakcı E. Musculoskeletal pain and its relation to individual and work-related factors: A cross-sectional study among Turkish office workers who work using computers. Int J Occup Saf Ergon. 2020;28(2):790-7. [DOI] [PMID]
38. Jaroenrungsup Y, Kanchanomai S, Khruakhorn S. Effects of self-posture correction exercise in forward head posture of smartphone users. J Sci Technol. 2021;43(2):439. [Article]
39. O'Riordan C, Clifford A, Van De Ven P, Nelson J. Chronic neck pain and exercise interventions: frequency, intensity, time, and type principle. Arch Phys Med Rehabil. 2014;95(4):770-83. [DOI] [PMID]
40. Sarraf F, Abbasi S, Varmazyar S. Self-Management Exercises Intervention on Text Neck Syndrome Among University Students Using Smartphones. Pain Manag Nurs. 2023;24(6):595-602. [DOI] [PMID]
41. Valipour Noroozi M, Hajibabaei M, Saki A, Memari Z. Prevalence of musculoskeletal disorders among office workers. Jundishapur J Health Sci. 2015;7(1):e27157. [DOI]
42. Fortún-Rabadán R, Jiménez-Sánchez C, Flores-Yaben O, Bellosta-López P. Workplace physiotherapy for musculoskeletal pain-relief in office workers: A pilot study. J Educ Health Promot. 2021;10:75. [DOI] [PMID] [PMCID]
43. Kelly D, Shorthouse F, Roffi V, Tack C. Exercise therapy and work-related musculoskeletal disorders in sedentary workers. Occup Med (Lond). 2018;68(4):262-72. [DOI] [PMID]
44. Andersen LL, Christensen KB, Holtermann A, Poulsen OM, Sjøgaard G, Pedersen MT, et al. Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: a one-year randomized controlled trial. Man Ther. 2010;15(1):100-4. [DOI] [PMID]
45. Mehtab S, Zamurd N. Comparison of isometric neck exercises and stretching with ergonomic modifications versus isometric neck exercises and stretching for mechanical neck pain: A randomized controlled trail: J Riphah Coll Rehabil Sci. 2019;7(1):7-11. [Article]
46. Im B, Kim Y, Chung Y, Hwang S. Effects of scapular stabilization exercise on neck posture and muscle activation in individuals with neck pain and forward head posture. J Phys Ther Sci. 2016;28(3):951-5. [DOI] [PMID] [PMCID]
47. Kang NY, Im SC, Kim K. Effects of a combination of scapular stabilization and thoracic extension exercises for office workers with forward head posture on the craniovertebral angle, respiration, pain, and disability: A randomized-controlled trial. Turk J Phys Med Rehabil. 2021;67(3):291-9. [DOI] [PMID] [PMCID]
48. Lee J, Lee M, Lim T, Kim T, Kim S, Suh D, et al. Effectiveness of an application-based neck exercise as a pain management tool for office workers with chronic neck pain and functional disability: a pilot randomized trial. Eur J Integr Med. 2017;12:87-92. [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution 4.0 International License. |
