Journal of Occupational
Health and Epidemiology

Rafsanjan university Of medical sciences
Volume 13, Issue 3 (Summer 2024)
J Occup Health Epidemiol 2024, 13(3): 157-165 |
Back to browse issues page


Ethics code: IR.MAZUMS.REC.1401.228
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Pouramanyan Hir M, Nasiri-Formi E, Akbari F, Rosgard B. Comparison of the Effects of Inhaling Citrus Aurantium Essential Oil and Stretching Exercises on Fatigue of Operating Room Personnel. J Occup Health Epidemiol 2024; 13 (3) :157-165
URL: http://johe.rums.ac.ir/article-1-771-en.html
URL: http://johe.rums.ac.ir/article-1-771-en.html
Related article in
Google Scholar
Google Scholar
Similar articles



1- 1. M.Sc. in Operating Room, Dept. of Anesthesia and Operating Room, Master's student of Operating Room, Student Research Committee, School of Allied Medical Sciences, Mazandaran University of Medical Sciences, Sari, Iran.
2- Associate Prof., Dept. of Anesthesiology, Operating Room, School of Allied Medical Sciences, Traditional and Complementary Medicine Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran. ,rezanf2002@yahoo.com
3- M.D. in Sports Medicine, Imam Ali hospital, Mazandaran University of Medical Sciences, Amol, Iran.
4- M.Sc. in Operating Room, Dept. of Anesthesia and Operating Room, Master's Student in Operating Room, Student Research Committee, School of Allied Medical Sciences, Mazandaran University of Medical Sciences, Sari, Iran.
2- Associate Prof., Dept. of Anesthesiology, Operating Room, School of Allied Medical Sciences, Traditional and Complementary Medicine Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran. ,
3- M.D. in Sports Medicine, Imam Ali hospital, Mazandaran University of Medical Sciences, Amol, Iran.
4- M.Sc. in Operating Room, Dept. of Anesthesia and Operating Room, Master's Student in Operating Room, Student Research Committee, School of Allied Medical Sciences, Mazandaran University of Medical Sciences, Sari, Iran.
Article history

Received: 2023/09/7
Accepted: 2024/07/15
ePublished: 2024/09/28
Accepted: 2024/07/15
ePublished: 2024/09/28
Subject:
Occupational Health
Full-Text [PDF 380 kb]
(122 Downloads)
| Abstract (HTML) (325 Views)
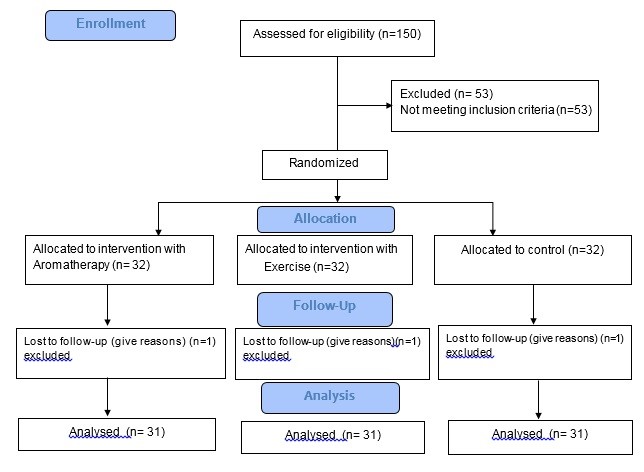
Table 1. Mean comparison of fatigue levels among three groups before as well as 2, 4, and 6 weeks post-intervention
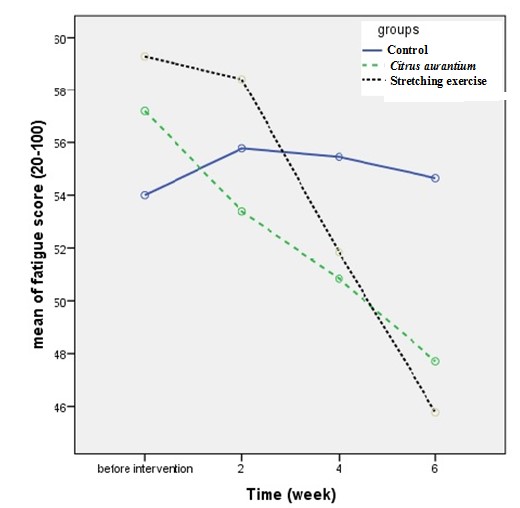
Fig. 2. Mean fatigue change in the three groups during study
Full-Text: (72 Views)
Introduction
The term "fatigue" refers to the temporary inability to maintain muscle power or strength during successive contractions, as well as a feeling of physical and mental incapacity. Additionally, feelings of discomfort, failure, and humiliation can be evident in an affected person [1]. One effect of job-related fatigue is a decline in performance. Job performance is defined as the degree to which a person performs tasks assigned to them in their job, and good performance can boost organizational productivity. This, in turn, can promote the national economy of society [2].
Nurses work in various departments and areas of the hospital. Meanwhile, operating room staff are also an integral part of the nursing community. Due to the demanding nature of their job, they are susceptible to various stresses that may lead to burnout and fatigue. This can further result in a desire to quit and provide suboptimal patient care [3].
Surgical technologists and operating room nurses working the night shift should be prepared to receive emergency patients, such as those who have been in accidents, at any time [4]. Studies have shown that around 50% of nurses suffer from chronic fatigue [5]. Johnson's research, which is consistent with other studies, reports that around 50% of nurses experience fatigue. Furthermore, out of approximately 50 to 90% of nurses working in healthcare centers, about 90% of nurses working in hospitals suffer from fatigue [5,6].
In Iran, the level of fatigue among operating room staff and nurses is higher compared to other staff [6]. The findings indicated significant levels of fatigue across various domains, overall fatigue subjective fatigue, concentration, motivation, and physical activity scoring at 48.73%, 54.31%, 51.65%, 38.96%, and 42.06% respectively [6-7].
Various solutions have been proposed and confirmed in many previous studies to prevent and eliminate fatigue. One such solution is exercise, which has been used in research to eliminate and reduce fatigue. Based on the results of some studies, it was shown that some types of exercise such as aerobic exercise can have positive effects on reducing the feeling of patient fatigue (7-10). According to Harma et al.'s study (1988), exercise reduces fatigue [7]. Furthermore, several studies have shown that aerobic exercise [8], particularly stretching exercises, can help reduce fatigue in patients suffering from fibromyalgia [9] and multiple sclerosis [10].
However, despite its benefits, the results show that about 90% of nurses do not exercise regularly once a week [11]. Some studies have also mentioned the effect of exercise on the fatigue of chronic patients, and it is considered the most effective non-pharmacological method for relieving fatigue and even preventing diseases. Exercise can create physiological adaptations that improve the efficiency of the system, energy levels, and boost overall performance ability [12].
Aromatherapy, a holistic healing approach utilizing plant extracts, enhances well-being by engaging the limbic system in the brain. This system, governing emotions, behaviors, and memory, interacts with aromatic compounds to alleviate fatigue. Inhaling or applying essential oils activates the olfactory system, influencing mood, stress, and fatigue levels through brain signaling. Citrus aurantium essential oil comes from the Rutaceae family and has a soothing fragrance which is recommended in written sources of Iranian traditional medicine for its ability to calm and strengthen the heart. This essential oil is known to have therapeutic properties such as reducing stress and anxiety, improving mood, and promoting relaxation. Additionally, its pleasant aroma is believed to positively impact mental health and well-being. Citrus aurantium essential oil can be used in various ways including aromatherapy, massage, and as an ingredient in skincare products. Aromatherapy is considered one of the complementary or alternative treatment methods that are believed to be effective in relieving pain, reducing worry and anxiety, insomnia, depression, fatigue, asthma, and more [5]. It involves the controlled use of aromatic oils to maintain and promote physical and mental health and is used as a part of nursing in many countries, including Switzerland, Germany, England, Canada, and America [13].
Inhaling the scent from essential oils can shift the autonomic balance towards parasympathetic activity, promoting relaxation and calmness [14]. This method has been found to be particularly effective in reducing stress and anxiety levels among patients.
Due to high work pressure and the prevalence of fatigue, no specific interventions have been made thus far. Various studies propose new techniques to reduce fatigue [15].
Surgical technologists in operating rooms are more likely to experience fatigue due to the special and stressful conditions as well as the variety and sensitivity of surgical procedures. This fatigue can affect the quality of surgical procedures and patient care before and during operation. While drug use has been proposed to prevent and relieve fatigue, researchers are now exploring non-pharmaceutical methods, such as exercise and aromatherapy in various fields [16].
The present study aims to compare the effects of inhaling Citrus aurantium scent, stretching exercises, and a combination of both on the fatigue of operating room personnel in Amol educational and therapeutic hospitals.
Materials and Methods
The present study was an Interventional study conducted on operating room personnel working in educational and therapeutic hospitals in Amol city. The study population in this research consisted of all operating room personnel of hospitals in Amol city who met the inclusion and exclusion criteria.
The inclusion criteria included: written informed consent, experiencing mild or higher levels of fatigue, having at least one year of experience working in the operating room, and possessing a healthy sense of smell. The exclusion criteria for this study were: having a history of accidents or traumatic injuries, no history of participating in regular professional sports programs within the last year, having a medical restriction that would prevent them from performing stretching exercises, sensitivity to the Citrus aurantium, and having a history of allergic asthma. We used the following formula to estimate the sample size, with variances (σ1 = 7.3 and σ2 = 6.7), mean difference = 5, alpha error = 0.05, and test power equal to 80% respectively. The sample size was estimated using the formula for comparing means of fatigue in independent groups, based on the study by Zadi and colleagues [16], which determined a sample size of 29 individuals. To enhance the study's accuracy and account for sample loss, 10% was added, resulting in 32 individuals in each group. The parameters and formula are as follows.
Formula 1.

In this clinical trial with three groups (Citrus, exercise, and control) and 32 patients per group, the randomization process using block randomization can be described as follows: participants are divided into blocks of 6, with 16 blocks in total, each containing a balanced distribution of treatments. For each block, such as AABBCC, AABCBC, AACBBC, etc., one sequence was randomly selected, and the treatments were assigned to the participants accordingly. This process was repeated for all 16 blocks, ensuring a balanced distribution of treatments and minimizing bias in the study. Four participants continued involuntarily after randomization (Fig. 1). To conceal the type of intervention, 96 opaque envelopes were utilized, with each envelope labeled on the outside with the corresponding patient's registration number, while the type of intervention was enclosed within the envelope. Data collectors were unaware of the assigned intervention. One participant from the Citrus aroma group, two from the exercise group, and one from the control group withdrew due to personal desire after randomization.
The data collection tool consisted of a questionnaire with two parts: demographic information and a fatigue measurement questionnaire.
The demographic characteristics questionnaire included questions about age, weight, marital status, number of children, work experience in the operating room department, education level, employment status, shift work status, number of overtime hours per month, number of sleep hours per 24 hours, history of systemic disease, history of regular exercise program, and gender.
The Multidimensional Fatigue Inventory (MFI): the multidimensional fatigue measurement standard questionnaire consisted of 20 items evaluating five dimensions of fatigue, including general fatigue, physical fatigue, mental fatigue, decreased activity, and decreased motivation. This questionnaire provided a deeper and more accurate understanding of a person's fatigue level. The questionnaire is graded based on a 5-point Likert scale, ranging from one (completely true) to five (completely false). Each dimension of the questionnaire consists of four questions, and the answers are collected on a scale of five options. The total score of the fatigue questionnaire falls within the range of 20 to 100. The scoring system for fatigue severity is as follows: a score of 20-46 indicates mild fatigue, 47-73 reveals moderate fatigue, and 74-100 indicates severe fatigue. This questionnaire was first developed by Smith and colleagues in 1996. Its validity and reliability have been evaluated in various demographic groups, including patients suffering from different diseases or chronic fatigue syndrome. In a study conducted by Zadi et al. in Iran, it was reported that the validity and reliability of this questionnaire were confirmed in several studies in Iran. Further, the questionnaire has good internal consistency, Cronbach's alpha coefficient for the areas of general fatigue, physical fatigue, and mental fatigue was equal to or greater than 80%, indicating strong reliability. For the areas of decreased motivation and decreased activity, the coefficient was above 60%, suggesting acceptable reliability.
The validity of the questionnaire was confirmed according to previous similar studies [5, 16-20]. In the present study, the reliability of this tool was rechecked using Cronbach's alpha coefficient, and it was estimated at 82%. The Pearson correlation coefficient between the first week and the next two weeks was equal to 693%, (p<0.001). After obtaining the necessary permits from the Research and Technology Vice-Chancellor and the Ethics Committee of Mazandaran University of Medical Sciences under the number IR.MAZUMS.REC.1401.22, the researcher coordinated with affiliated hospitals and visited the operating room departments of Amol hospitals during three shifts to collect samples.
Initially, the questionnaire was distributed among 150 eligible operating room personnel. Based on the MFI fatigue measurement scale, 96 operating room personnel who reported mild to high levels of fatigue intensity were selected for the study. They were assigned to three groups through a simple random method for intervention. In each group, one participant discontinued after randomization. Accordingly, 93 individuals were analyzed (Fig. 1).
In this study, the control group did not receive any intervention, and only assessments were conducted throughout the study period. In the exercise group, a stretching exercise program was implemented. The term "stretching exercise" in this study refers to performing stretching movements tailored to the work environment and operating room, as adjusted by a sports medicine specialist. The researcher provided face-to-face training on the technique of stretching exercises to the operating room personnel. To perform the combined exercise techniques, the participants were instructed to exercise during their work shift and free time in a relatively quiet environment while remaining in a relaxed state. They were asked to perform these exercises once in every shift for 10 minutes. One of the researchers supervised this process until the end of the study. Stretching exercises were performed for ten minutes, during free time and at the beginning of the shift and before surgery, four times a week and once a day. Six stretching sports movements were coded as follows:
a. Waist stretch (forward): Stand straight with your knees extended and bend forward at the waist. Extend your arms towards the ground. Hold for 1 minute.
b. Waist stretch (side): Stand straight with your knees extended and bend your upper limbs to one side up to the waist area. Place your hands along your legs.
Repeat for the opposite side. Hold each side for 1 minute, totaling 2 minutes.
c. Waist stretch (backward): Stand straight with your knees extended and move your upper limbs along with your hands backward. Create tension and rotate your hands with the upper body. Perform this movement once to the right and once to the left. Hold each side for 1 minute, totaling 2 minutes.
d. Shoulder stretch (upwards): Stand straight and stretch your hands from the shoulder area upwards and in front of your face. Keep your elbows slightly bent and aligned with your chin and nose, with your palms interlocked at the top.
e. Shoulder stretch (backwards): Stand straight and connect both your hands from behind in opposite directions (right hand from above and left hand from below). Place them in a stretching position and move them for the next stretching of the hands. Hold for 2 minutes.
f. Shoulder stretch (rotating): Stand straight and stretch both your hands so that your palms are stuck together above your head. Rotate them for a maximum of 180 degrees for 30 seconds.
Repeat for 2 minutes.
In the Citrus aurantium essential oil and scent group, a neck pendant containing Orange Spring essential oil was provided to the participants. The pendant consisted of a container containing cotton soaked with three drops of Orange Spring essential oil, which had a concentration of 10% and was produced by Abaid Chemical Company in Iran. The pendant was placed in front of the chest and positioned at a distance of 20 cm from the nose. The personnel were instructed to inhale the scent for 20 minutes during each work shift.
The participants in the aromatherapy group were asked not to use perfume or cologne on the day of intervention. The interventions (inhaling the scent of Citrus aurantium and performing stretching exercises) were repeated twice in each shift during the week. At the end of the week, the participants completed the fatigue assessment questionnaire. Fatigue was measured in seven stages, including the preliminary stage (before the intervention to determine individuals with mild or severe fatigue) and the stage at the end of the second week to the end of the sixth week, which were completed in a self-administered manner by all three groups.
After collecting the data, the Kolmogorov-Smirnov test was employed to assess the normality of the distribution. If the distribution was normal, appropriate parametric tests such as ANOVA statistical tests were used. Otherwise, the corresponding non-parametric tests such as Kruskal-Wallis were utilized.
The amount of fatigue, which was measured at four time steps, was analyzed using a repeated measures test. Mean and standard deviation were used to describe the quantitative findings, while frequency and percentage were employed for the qualitative findings. The results were reported using a combination of text, tables, and graphs. The SPSS 20 software was used. A significant level of P<0.05 was considered for the analysis.
Results
Out of 150 operating room personnel examined, 96 eligible individuals were included in the study, divided into three groups. During the second and third week of the study, four participants from the aromatherapy, control, and fitness groups were excluded due to their unwillingness to continue cooperation. However, 93 participants continued to cooperate with the researchers until the end of the study (Fig. 1).
The research findings revealed that out of the 93 subjects, 16 (17.2%) were male and 77 (82.8%) were female. Additionally, it was revealed that 70 people (75.3%) were married, while 23 people (24.7%) were single. The mean age of the participants was 34.35 ± 7.23, with an average work experience of 9.35 ± 6.65 and an average body mass index of 25.68 ± 4.2. Of the participants, 72 (77.4%) had a bachelor's degree, 10 (10.8%) held an associate degree,7 (7.5%) held a diploma, and 4 (4.3%) held a master's degree. Results from statistical tests indicated that there were no significant differences between the demographic characteristics of the participants in terms of age, marital status, education level, and body mass index across the three groups (p > 0.05).
The exercise group had a pre-intervention average fatigue score of 61.1±11.13, the control group 54.00±15.16, and the Citrus group 57.19±11.47 (p<0.095).
After four weeks post-intervention, the average fatigue intensity was 55.45±10.26 in the control group, 50.84±12.73 in the Citrus group, and 51.84±11.48 in the exercise group (p <0.259). After six weeks, the average fatigue intensity was 54.62±12.2 in the control group, 47.71±11.11 in the aroma group, and 45.77±11.7 in the exercise group (p <0.009) (Table 1). These results suggest that stretching exercises and aromatherapy can reduce fatigue intensity in the populations.
Repeated measured test revealed that each group has a significant difference in terms of fatigue compared to the previous one (p<0.001). In our current study, the average fatigue score dropped by 1.5% in the control group, 6.04% in the aroma group, and 11.7% in the stretching exercise group after 6 weeks (Table 1). The results showed that there were no significant differences in different stages within the control group or between the groups during the pre-intervention phase. Fig. 2 illustrates the results by groups and at different times.
The term "fatigue" refers to the temporary inability to maintain muscle power or strength during successive contractions, as well as a feeling of physical and mental incapacity. Additionally, feelings of discomfort, failure, and humiliation can be evident in an affected person [1]. One effect of job-related fatigue is a decline in performance. Job performance is defined as the degree to which a person performs tasks assigned to them in their job, and good performance can boost organizational productivity. This, in turn, can promote the national economy of society [2].
Nurses work in various departments and areas of the hospital. Meanwhile, operating room staff are also an integral part of the nursing community. Due to the demanding nature of their job, they are susceptible to various stresses that may lead to burnout and fatigue. This can further result in a desire to quit and provide suboptimal patient care [3].
Surgical technologists and operating room nurses working the night shift should be prepared to receive emergency patients, such as those who have been in accidents, at any time [4]. Studies have shown that around 50% of nurses suffer from chronic fatigue [5]. Johnson's research, which is consistent with other studies, reports that around 50% of nurses experience fatigue. Furthermore, out of approximately 50 to 90% of nurses working in healthcare centers, about 90% of nurses working in hospitals suffer from fatigue [5,6].
In Iran, the level of fatigue among operating room staff and nurses is higher compared to other staff [6]. The findings indicated significant levels of fatigue across various domains, overall fatigue subjective fatigue, concentration, motivation, and physical activity scoring at 48.73%, 54.31%, 51.65%, 38.96%, and 42.06% respectively [6-7].
Various solutions have been proposed and confirmed in many previous studies to prevent and eliminate fatigue. One such solution is exercise, which has been used in research to eliminate and reduce fatigue. Based on the results of some studies, it was shown that some types of exercise such as aerobic exercise can have positive effects on reducing the feeling of patient fatigue (7-10). According to Harma et al.'s study (1988), exercise reduces fatigue [7]. Furthermore, several studies have shown that aerobic exercise [8], particularly stretching exercises, can help reduce fatigue in patients suffering from fibromyalgia [9] and multiple sclerosis [10].
However, despite its benefits, the results show that about 90% of nurses do not exercise regularly once a week [11]. Some studies have also mentioned the effect of exercise on the fatigue of chronic patients, and it is considered the most effective non-pharmacological method for relieving fatigue and even preventing diseases. Exercise can create physiological adaptations that improve the efficiency of the system, energy levels, and boost overall performance ability [12].
Aromatherapy, a holistic healing approach utilizing plant extracts, enhances well-being by engaging the limbic system in the brain. This system, governing emotions, behaviors, and memory, interacts with aromatic compounds to alleviate fatigue. Inhaling or applying essential oils activates the olfactory system, influencing mood, stress, and fatigue levels through brain signaling. Citrus aurantium essential oil comes from the Rutaceae family and has a soothing fragrance which is recommended in written sources of Iranian traditional medicine for its ability to calm and strengthen the heart. This essential oil is known to have therapeutic properties such as reducing stress and anxiety, improving mood, and promoting relaxation. Additionally, its pleasant aroma is believed to positively impact mental health and well-being. Citrus aurantium essential oil can be used in various ways including aromatherapy, massage, and as an ingredient in skincare products. Aromatherapy is considered one of the complementary or alternative treatment methods that are believed to be effective in relieving pain, reducing worry and anxiety, insomnia, depression, fatigue, asthma, and more [5]. It involves the controlled use of aromatic oils to maintain and promote physical and mental health and is used as a part of nursing in many countries, including Switzerland, Germany, England, Canada, and America [13].
Inhaling the scent from essential oils can shift the autonomic balance towards parasympathetic activity, promoting relaxation and calmness [14]. This method has been found to be particularly effective in reducing stress and anxiety levels among patients.
Due to high work pressure and the prevalence of fatigue, no specific interventions have been made thus far. Various studies propose new techniques to reduce fatigue [15].
Surgical technologists in operating rooms are more likely to experience fatigue due to the special and stressful conditions as well as the variety and sensitivity of surgical procedures. This fatigue can affect the quality of surgical procedures and patient care before and during operation. While drug use has been proposed to prevent and relieve fatigue, researchers are now exploring non-pharmaceutical methods, such as exercise and aromatherapy in various fields [16].
The present study aims to compare the effects of inhaling Citrus aurantium scent, stretching exercises, and a combination of both on the fatigue of operating room personnel in Amol educational and therapeutic hospitals.
Materials and Methods
The present study was an Interventional study conducted on operating room personnel working in educational and therapeutic hospitals in Amol city. The study population in this research consisted of all operating room personnel of hospitals in Amol city who met the inclusion and exclusion criteria.
The inclusion criteria included: written informed consent, experiencing mild or higher levels of fatigue, having at least one year of experience working in the operating room, and possessing a healthy sense of smell. The exclusion criteria for this study were: having a history of accidents or traumatic injuries, no history of participating in regular professional sports programs within the last year, having a medical restriction that would prevent them from performing stretching exercises, sensitivity to the Citrus aurantium, and having a history of allergic asthma. We used the following formula to estimate the sample size, with variances (σ1 = 7.3 and σ2 = 6.7), mean difference = 5, alpha error = 0.05, and test power equal to 80% respectively. The sample size was estimated using the formula for comparing means of fatigue in independent groups, based on the study by Zadi and colleagues [16], which determined a sample size of 29 individuals. To enhance the study's accuracy and account for sample loss, 10% was added, resulting in 32 individuals in each group. The parameters and formula are as follows.
Formula 1.
In this clinical trial with three groups (Citrus, exercise, and control) and 32 patients per group, the randomization process using block randomization can be described as follows: participants are divided into blocks of 6, with 16 blocks in total, each containing a balanced distribution of treatments. For each block, such as AABBCC, AABCBC, AACBBC, etc., one sequence was randomly selected, and the treatments were assigned to the participants accordingly. This process was repeated for all 16 blocks, ensuring a balanced distribution of treatments and minimizing bias in the study. Four participants continued involuntarily after randomization (Fig. 1). To conceal the type of intervention, 96 opaque envelopes were utilized, with each envelope labeled on the outside with the corresponding patient's registration number, while the type of intervention was enclosed within the envelope. Data collectors were unaware of the assigned intervention. One participant from the Citrus aroma group, two from the exercise group, and one from the control group withdrew due to personal desire after randomization.
The data collection tool consisted of a questionnaire with two parts: demographic information and a fatigue measurement questionnaire.
The demographic characteristics questionnaire included questions about age, weight, marital status, number of children, work experience in the operating room department, education level, employment status, shift work status, number of overtime hours per month, number of sleep hours per 24 hours, history of systemic disease, history of regular exercise program, and gender.
The Multidimensional Fatigue Inventory (MFI): the multidimensional fatigue measurement standard questionnaire consisted of 20 items evaluating five dimensions of fatigue, including general fatigue, physical fatigue, mental fatigue, decreased activity, and decreased motivation. This questionnaire provided a deeper and more accurate understanding of a person's fatigue level. The questionnaire is graded based on a 5-point Likert scale, ranging from one (completely true) to five (completely false). Each dimension of the questionnaire consists of four questions, and the answers are collected on a scale of five options. The total score of the fatigue questionnaire falls within the range of 20 to 100. The scoring system for fatigue severity is as follows: a score of 20-46 indicates mild fatigue, 47-73 reveals moderate fatigue, and 74-100 indicates severe fatigue. This questionnaire was first developed by Smith and colleagues in 1996. Its validity and reliability have been evaluated in various demographic groups, including patients suffering from different diseases or chronic fatigue syndrome. In a study conducted by Zadi et al. in Iran, it was reported that the validity and reliability of this questionnaire were confirmed in several studies in Iran. Further, the questionnaire has good internal consistency, Cronbach's alpha coefficient for the areas of general fatigue, physical fatigue, and mental fatigue was equal to or greater than 80%, indicating strong reliability. For the areas of decreased motivation and decreased activity, the coefficient was above 60%, suggesting acceptable reliability.
The validity of the questionnaire was confirmed according to previous similar studies [5, 16-20]. In the present study, the reliability of this tool was rechecked using Cronbach's alpha coefficient, and it was estimated at 82%. The Pearson correlation coefficient between the first week and the next two weeks was equal to 693%, (p<0.001). After obtaining the necessary permits from the Research and Technology Vice-Chancellor and the Ethics Committee of Mazandaran University of Medical Sciences under the number IR.MAZUMS.REC.1401.22, the researcher coordinated with affiliated hospitals and visited the operating room departments of Amol hospitals during three shifts to collect samples.
Initially, the questionnaire was distributed among 150 eligible operating room personnel. Based on the MFI fatigue measurement scale, 96 operating room personnel who reported mild to high levels of fatigue intensity were selected for the study. They were assigned to three groups through a simple random method for intervention. In each group, one participant discontinued after randomization. Accordingly, 93 individuals were analyzed (Fig. 1).
In this study, the control group did not receive any intervention, and only assessments were conducted throughout the study period. In the exercise group, a stretching exercise program was implemented. The term "stretching exercise" in this study refers to performing stretching movements tailored to the work environment and operating room, as adjusted by a sports medicine specialist. The researcher provided face-to-face training on the technique of stretching exercises to the operating room personnel. To perform the combined exercise techniques, the participants were instructed to exercise during their work shift and free time in a relatively quiet environment while remaining in a relaxed state. They were asked to perform these exercises once in every shift for 10 minutes. One of the researchers supervised this process until the end of the study. Stretching exercises were performed for ten minutes, during free time and at the beginning of the shift and before surgery, four times a week and once a day. Six stretching sports movements were coded as follows:
a. Waist stretch (forward): Stand straight with your knees extended and bend forward at the waist. Extend your arms towards the ground. Hold for 1 minute.
b. Waist stretch (side): Stand straight with your knees extended and bend your upper limbs to one side up to the waist area. Place your hands along your legs.
Repeat for the opposite side. Hold each side for 1 minute, totaling 2 minutes.
c. Waist stretch (backward): Stand straight with your knees extended and move your upper limbs along with your hands backward. Create tension and rotate your hands with the upper body. Perform this movement once to the right and once to the left. Hold each side for 1 minute, totaling 2 minutes.
d. Shoulder stretch (upwards): Stand straight and stretch your hands from the shoulder area upwards and in front of your face. Keep your elbows slightly bent and aligned with your chin and nose, with your palms interlocked at the top.
e. Shoulder stretch (backwards): Stand straight and connect both your hands from behind in opposite directions (right hand from above and left hand from below). Place them in a stretching position and move them for the next stretching of the hands. Hold for 2 minutes.
f. Shoulder stretch (rotating): Stand straight and stretch both your hands so that your palms are stuck together above your head. Rotate them for a maximum of 180 degrees for 30 seconds.
Repeat for 2 minutes.
In the Citrus aurantium essential oil and scent group, a neck pendant containing Orange Spring essential oil was provided to the participants. The pendant consisted of a container containing cotton soaked with three drops of Orange Spring essential oil, which had a concentration of 10% and was produced by Abaid Chemical Company in Iran. The pendant was placed in front of the chest and positioned at a distance of 20 cm from the nose. The personnel were instructed to inhale the scent for 20 minutes during each work shift.
The participants in the aromatherapy group were asked not to use perfume or cologne on the day of intervention. The interventions (inhaling the scent of Citrus aurantium and performing stretching exercises) were repeated twice in each shift during the week. At the end of the week, the participants completed the fatigue assessment questionnaire. Fatigue was measured in seven stages, including the preliminary stage (before the intervention to determine individuals with mild or severe fatigue) and the stage at the end of the second week to the end of the sixth week, which were completed in a self-administered manner by all three groups.
After collecting the data, the Kolmogorov-Smirnov test was employed to assess the normality of the distribution. If the distribution was normal, appropriate parametric tests such as ANOVA statistical tests were used. Otherwise, the corresponding non-parametric tests such as Kruskal-Wallis were utilized.
The amount of fatigue, which was measured at four time steps, was analyzed using a repeated measures test. Mean and standard deviation were used to describe the quantitative findings, while frequency and percentage were employed for the qualitative findings. The results were reported using a combination of text, tables, and graphs. The SPSS 20 software was used. A significant level of P<0.05 was considered for the analysis.
Results
Out of 150 operating room personnel examined, 96 eligible individuals were included in the study, divided into three groups. During the second and third week of the study, four participants from the aromatherapy, control, and fitness groups were excluded due to their unwillingness to continue cooperation. However, 93 participants continued to cooperate with the researchers until the end of the study (Fig. 1).
The research findings revealed that out of the 93 subjects, 16 (17.2%) were male and 77 (82.8%) were female. Additionally, it was revealed that 70 people (75.3%) were married, while 23 people (24.7%) were single. The mean age of the participants was 34.35 ± 7.23, with an average work experience of 9.35 ± 6.65 and an average body mass index of 25.68 ± 4.2. Of the participants, 72 (77.4%) had a bachelor's degree, 10 (10.8%) held an associate degree,7 (7.5%) held a diploma, and 4 (4.3%) held a master's degree. Results from statistical tests indicated that there were no significant differences between the demographic characteristics of the participants in terms of age, marital status, education level, and body mass index across the three groups (p > 0.05).
The exercise group had a pre-intervention average fatigue score of 61.1±11.13, the control group 54.00±15.16, and the Citrus group 57.19±11.47 (p<0.095).
After four weeks post-intervention, the average fatigue intensity was 55.45±10.26 in the control group, 50.84±12.73 in the Citrus group, and 51.84±11.48 in the exercise group (p <0.259). After six weeks, the average fatigue intensity was 54.62±12.2 in the control group, 47.71±11.11 in the aroma group, and 45.77±11.7 in the exercise group (p <0.009) (Table 1). These results suggest that stretching exercises and aromatherapy can reduce fatigue intensity in the populations.
Repeated measured test revealed that each group has a significant difference in terms of fatigue compared to the previous one (p<0.001). In our current study, the average fatigue score dropped by 1.5% in the control group, 6.04% in the aroma group, and 11.7% in the stretching exercise group after 6 weeks (Table 1). The results showed that there were no significant differences in different stages within the control group or between the groups during the pre-intervention phase. Fig. 2 illustrates the results by groups and at different times.
Fig. 1. CONSORT 2010 Flow Diagram
The results of the analysis of variance test in repeated measurements indicated that there was no significant difference at different times in the control group. In contrast, significant differences were observed in the scent and exercise groups in the weeks after the intervention compared to pre-intervention (P<0.01). The fatigue index in the scent group dropped significantly at 4 and 6 weeks after the intervention compared to the initial stage (P=0.024, P=0.006, respectively), while it did not reach a significant level at 2 weeks after the activity (P=0.051). The results also demonstrated that the fatigue index in the exercise group declined significantly at 2, 4, and 6 weeks after the exercise intervention compared to the pre-test (P=0.007, P=0.000, P=0.004, respectively). No differences were observed in the control group at different stages (P=0.34, P=0.606, P=0.433, respectively). Before the intervention, the fatigue index in the control group was higher than in the other groups (Table 1).
Table 1. Mean comparison of fatigue levels among three groups before as well as 2, 4, and 6 weeks post-intervention
| Group | Before intervention | 2 weeks | 4 weeks | 6 weeks | Repeated measure |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Control | 54±15.17 | 55.77±10.42 | 55.45±10.26 | 54.62±12.2 | P<0.34 |
| Citrus | 57.19±11.47 | 53.39±11.79 | 50.84±12.73 | 47.71±11.11 | P<0.001 |
| Rxercise | 61.1±11.13 | 58.42±12.06 | 51.84±11.48 | 45.77±11.71 | P<0.001 |
| ANOVA | P<0.095 | P<0.229 | P<0.259 | P<0.009 |
Fig. 2. Mean fatigue change in the three groups during study
Discussion
The present study aimed to examine the effects of stretching exercises and inhalation of Baharnaranj on the severity of fatigue among operating room personnel. Both stretching exercises and Baharnaranj essential oil were effective in reducing fatigue. However, the exercise group showed a greater reduction in fatigue intensity compared to the Baharnaranj group, while the control group reported no change in fatigue levels.
These findings underscore the positive impact of stretching exercises on mitigating fatigue among operating room personnel. They align with previous studies by Taha et al., Aristotle et al., Jam Bersang et al., and Pazukian et al., while being at odds with the results of Surakka et al. and Doring et al. Other studies also support the findings of the present study [5, 18-22]. In Taha et al.'s study, regarding the difference in fatigue levels between the two groups, 57.5% of participants in the exercise group experienced moderate to severe fatigue, while 100% in the control group reported fatigue. In this study, it was shown that deep breathing and exercise were effective on reducing fatigue intensity in women with breast cancer, with a greater reduction in the intervention group compared to the control group [18].
In the before and after study by Behbodi et al., it was reported that the intensity of fatigue, with an average score of 6.54±0.43 in the pre-intervention phase, dropped to a score of 6.13±0.38 after 4 weeks of stretching exercise and to a score of 5.7±o.36 after 8 weeks (20). They concluded that stretching aerobic exercise could reduce the intensity of fatigue by 5% in 4 weeks and 6% after 8 weeks. The mentioned results were in line with the findings of our study. The outcomes of our present study have shown that the intensity of fatigue diminished by doing stretching exercise. In our current study, the average fatigue score decreased by 1.5% in the control group, 6.04% in the aroma group, and 11.7% in the stretching exercise group after 6 weeks. Research has shown that aerobic exercise can significantly reduce fatigue. The studies mentioned above align with our current study's findings, indicating that stretching exercises can reduce fatigue. However, our study also found that the use of inhaling the Citrus had effect on reducing fatigue.
Aristotle et al. [19] found that 6 weeks of aerobic exercise resulted in a significant reduction in fatigue among patients with multiple sclerosis. In another study, special care nurses experienced an 11.61% decline in fatigue levels post-exercise compared to before exercise [20]. Zadi Akhole et al. [16] reported a significant reduction in the severity of fatigue among operating room personnel after 6 weeks of combined exercise and inhalation of lavender essential oil.
However, Surakka et al. [21] concluded that a combined exercise program did not significantly alter the fatigue levels of multiple sclerosis patients. Similarly, Doring et al. [22] found that moderate-intensity exercise had little effect on fatigue.
The difference in the types and number of research units, the type of scale or tool used to measure fatigue, as well as the type, manner, and duration of exercise are some of the reasons behind the discrepancies in the results. Additionally, the existence of diseases and other background issues among research participants can also be effective on yielding contradictory results.
Based on the findings of this study, which was conducted on people without systemic disease, continuing with a few simple movements of stretching exercises promises to reduce fatigue during the intervention period and potentially bring about happiness.
With regards to the effect of orange spring scent on the fatigue of operating room personnel, the results of this study revealed that aromatherapy produces a significant reduction in the severity of fatigue among such personnel. The six-week aromatherapy intervention led to a significant decline in the level of fatigue experienced by operating room personnel compared to before the intervention. Further, the results of this study indicated a significant difference between the intervention groups and the control group in terms of fatigue.
The studies of other researchers that obtained similar results to the present research include those conducted by Naji SA et al. [23], M.I Jo [24], Park S et al. [25], Bahrami et al. [26], and Sakamoto et al. (27).
Naji SA research entitled ‘The Effect of Aromatherapy Massage on the Severity of Fatigue in Multiple Sclerosis Patients’ showed that aromatherapy massage has an effect on reducing the severity of fatigue [26]. In their study, Sakamoto et al. concluded that lavender essential oil improves concentration levels during work and mitigates fatigue by suppressing the sympathetic system [27].
Additionally, in a study conducted by Chang et al. to examine the effect of aromatherapy on the fatigue and sleep quality of nurses, they reported a positive effect of aromatherapy on reducing nurses' fatigue [28].
Although the characteristics of the samples examined in those studies differ from the participants in our study, the similar effects observed in all studies are likely related to the mechanism of aroma's relaxing properties, which were the same among the participants in the above research. In contrast to the results of a study conducted by Heeok Park et al. to determine the effect of aromatherapy massage on the level of fatigue of hospice patients in the final stages of their disease, they did not report a significant reduction in the level of fatigue, which is inconsistent with the results of the present study [29].
We can attribute the difference between the above research results and ours to several factors, including the small number of samples in the test group (17 people), the short duration of the study (five days), the low concentration of the essential oil (1%), and the characteristics of the participants in the study. These factors may have contributed to the emergence of different aroma effects.
One limitation of this research was the difficulty of measuring fatigue as it is a mental notion which can be influenced by variables such as emotional changes and job factors. Additionally, the lack of control over the mental state of the operating room personnel was another limitation, which could have affected the fatigue and the results of the study. To address this issue, the researchers asked the subjects not to undergo intervention on days when they were not in their usual physical and mental condition at the time of the intervention.
These two methods are recommended for operating room personnel who are exposed to chronic fatigue due to the sensitivities of surgical operations, the stressful environment of the operating room, physical limitations of the workspace, and prolonged standing. Therefore, the use of non-medicinal methods such as exercise and inhalation of spring orange essential oil is suggested as a strategy to reduce and prevent personnel fatigue.
Furthermore, since the positive effects of stretching exercise interventions were observed after two weeks and spring orange essential oil reduced fatigue after four weeks, it seems that continuing these interventions for longer periods in the operating room environment would be more effective. Accordingly, it is suggested that a research study be conducted using the survival analysis approach to investigate the long-term effectiveness of these interventions on mitigating fatigue among personnel in sensitive departments such as special care and emergency. These interventions should also be considered in management protocols for sensitive areas such as the operating room and anesthesia.
Conclusion
Performing stretching exercises and inhaling the scent of Citrus aurantium in the operating room had a favorable effect on the fatigue of the operating room personnel and lowered their fatigue. The stretching exercise program was easy to learn, and both interventions were low-cost, required minimal time, and did not have any complications.
Acknowledgement
We would like to thank the Honorable Vice President of Research and Technology of Mazandaran University of Medical Sciences, the Student Research Committee of Mazandaran University of Medical Sciences, and all participating operating room personnel.
Conflict of interest
None declared.
Funding
This research was carried out with the support of the Student Research and Technology Committee and the Deputy of Research and Technology of Mazandaran University of Medical Sciences with code 228-1401.
Ethical Considerations
This study has been in agreement with the Helsinki Declaration and Iranian national guidelines for ethics in research.
Code of Ethics
This study was conducted with the financial support of Mazandaran University of Medical Sciences (code: 1401-228) (Ethic code: IR.MAZUMS.REC.1401.228).
Authors' Contributions
Maryam Pouramanyan Hir: Design of the study, data collection, and analysis. Contributed to drafting the manuscript and Edited the manuscript, Read and approved the final version. Ebrahim Nasiri-Formi: conceptualization, Design of the study, a crucial role in overseeing the research process, guiding the statistical analysis, providing critical revisions, approved the final version. Faramarz Akbari: implementation of the intervention, data collection, data analysis and interpretation, Approved the final version. Bahareh Rozgard: data collection, reviewing literature, read and approved the final version.
The present study aimed to examine the effects of stretching exercises and inhalation of Baharnaranj on the severity of fatigue among operating room personnel. Both stretching exercises and Baharnaranj essential oil were effective in reducing fatigue. However, the exercise group showed a greater reduction in fatigue intensity compared to the Baharnaranj group, while the control group reported no change in fatigue levels.
These findings underscore the positive impact of stretching exercises on mitigating fatigue among operating room personnel. They align with previous studies by Taha et al., Aristotle et al., Jam Bersang et al., and Pazukian et al., while being at odds with the results of Surakka et al. and Doring et al. Other studies also support the findings of the present study [5, 18-22]. In Taha et al.'s study, regarding the difference in fatigue levels between the two groups, 57.5% of participants in the exercise group experienced moderate to severe fatigue, while 100% in the control group reported fatigue. In this study, it was shown that deep breathing and exercise were effective on reducing fatigue intensity in women with breast cancer, with a greater reduction in the intervention group compared to the control group [18].
In the before and after study by Behbodi et al., it was reported that the intensity of fatigue, with an average score of 6.54±0.43 in the pre-intervention phase, dropped to a score of 6.13±0.38 after 4 weeks of stretching exercise and to a score of 5.7±o.36 after 8 weeks (20). They concluded that stretching aerobic exercise could reduce the intensity of fatigue by 5% in 4 weeks and 6% after 8 weeks. The mentioned results were in line with the findings of our study. The outcomes of our present study have shown that the intensity of fatigue diminished by doing stretching exercise. In our current study, the average fatigue score decreased by 1.5% in the control group, 6.04% in the aroma group, and 11.7% in the stretching exercise group after 6 weeks. Research has shown that aerobic exercise can significantly reduce fatigue. The studies mentioned above align with our current study's findings, indicating that stretching exercises can reduce fatigue. However, our study also found that the use of inhaling the Citrus had effect on reducing fatigue.
Aristotle et al. [19] found that 6 weeks of aerobic exercise resulted in a significant reduction in fatigue among patients with multiple sclerosis. In another study, special care nurses experienced an 11.61% decline in fatigue levels post-exercise compared to before exercise [20]. Zadi Akhole et al. [16] reported a significant reduction in the severity of fatigue among operating room personnel after 6 weeks of combined exercise and inhalation of lavender essential oil.
However, Surakka et al. [21] concluded that a combined exercise program did not significantly alter the fatigue levels of multiple sclerosis patients. Similarly, Doring et al. [22] found that moderate-intensity exercise had little effect on fatigue.
The difference in the types and number of research units, the type of scale or tool used to measure fatigue, as well as the type, manner, and duration of exercise are some of the reasons behind the discrepancies in the results. Additionally, the existence of diseases and other background issues among research participants can also be effective on yielding contradictory results.
Based on the findings of this study, which was conducted on people without systemic disease, continuing with a few simple movements of stretching exercises promises to reduce fatigue during the intervention period and potentially bring about happiness.
With regards to the effect of orange spring scent on the fatigue of operating room personnel, the results of this study revealed that aromatherapy produces a significant reduction in the severity of fatigue among such personnel. The six-week aromatherapy intervention led to a significant decline in the level of fatigue experienced by operating room personnel compared to before the intervention. Further, the results of this study indicated a significant difference between the intervention groups and the control group in terms of fatigue.
The studies of other researchers that obtained similar results to the present research include those conducted by Naji SA et al. [23], M.I Jo [24], Park S et al. [25], Bahrami et al. [26], and Sakamoto et al. (27).
Naji SA research entitled ‘The Effect of Aromatherapy Massage on the Severity of Fatigue in Multiple Sclerosis Patients’ showed that aromatherapy massage has an effect on reducing the severity of fatigue [26]. In their study, Sakamoto et al. concluded that lavender essential oil improves concentration levels during work and mitigates fatigue by suppressing the sympathetic system [27].
Additionally, in a study conducted by Chang et al. to examine the effect of aromatherapy on the fatigue and sleep quality of nurses, they reported a positive effect of aromatherapy on reducing nurses' fatigue [28].
Although the characteristics of the samples examined in those studies differ from the participants in our study, the similar effects observed in all studies are likely related to the mechanism of aroma's relaxing properties, which were the same among the participants in the above research. In contrast to the results of a study conducted by Heeok Park et al. to determine the effect of aromatherapy massage on the level of fatigue of hospice patients in the final stages of their disease, they did not report a significant reduction in the level of fatigue, which is inconsistent with the results of the present study [29].
We can attribute the difference between the above research results and ours to several factors, including the small number of samples in the test group (17 people), the short duration of the study (five days), the low concentration of the essential oil (1%), and the characteristics of the participants in the study. These factors may have contributed to the emergence of different aroma effects.
One limitation of this research was the difficulty of measuring fatigue as it is a mental notion which can be influenced by variables such as emotional changes and job factors. Additionally, the lack of control over the mental state of the operating room personnel was another limitation, which could have affected the fatigue and the results of the study. To address this issue, the researchers asked the subjects not to undergo intervention on days when they were not in their usual physical and mental condition at the time of the intervention.
These two methods are recommended for operating room personnel who are exposed to chronic fatigue due to the sensitivities of surgical operations, the stressful environment of the operating room, physical limitations of the workspace, and prolonged standing. Therefore, the use of non-medicinal methods such as exercise and inhalation of spring orange essential oil is suggested as a strategy to reduce and prevent personnel fatigue.
Furthermore, since the positive effects of stretching exercise interventions were observed after two weeks and spring orange essential oil reduced fatigue after four weeks, it seems that continuing these interventions for longer periods in the operating room environment would be more effective. Accordingly, it is suggested that a research study be conducted using the survival analysis approach to investigate the long-term effectiveness of these interventions on mitigating fatigue among personnel in sensitive departments such as special care and emergency. These interventions should also be considered in management protocols for sensitive areas such as the operating room and anesthesia.
Conclusion
Performing stretching exercises and inhaling the scent of Citrus aurantium in the operating room had a favorable effect on the fatigue of the operating room personnel and lowered their fatigue. The stretching exercise program was easy to learn, and both interventions were low-cost, required minimal time, and did not have any complications.
Acknowledgement
We would like to thank the Honorable Vice President of Research and Technology of Mazandaran University of Medical Sciences, the Student Research Committee of Mazandaran University of Medical Sciences, and all participating operating room personnel.
Conflict of interest
None declared.
Funding
This research was carried out with the support of the Student Research and Technology Committee and the Deputy of Research and Technology of Mazandaran University of Medical Sciences with code 228-1401.
Ethical Considerations
This study has been in agreement with the Helsinki Declaration and Iranian national guidelines for ethics in research.
Code of Ethics
This study was conducted with the financial support of Mazandaran University of Medical Sciences (code: 1401-228) (Ethic code: IR.MAZUMS.REC.1401.228).
Authors' Contributions
Maryam Pouramanyan Hir: Design of the study, data collection, and analysis. Contributed to drafting the manuscript and Edited the manuscript, Read and approved the final version. Ebrahim Nasiri-Formi: conceptualization, Design of the study, a crucial role in overseeing the research process, guiding the statistical analysis, providing critical revisions, approved the final version. Faramarz Akbari: implementation of the intervention, data collection, data analysis and interpretation, Approved the final version. Bahareh Rozgard: data collection, reviewing literature, read and approved the final version.
References
1. Hooper C, Criag J, Janverin DR, Wetsel MA, Reimels E. Compassion Satisfaction, Burnout, and Compassion Fatigue Among Emergency Nurses Compared with Nurses in other Selected Inpatient Specialties. J Emerg Nurs. 2010;36(5):420-7. [DOI] [PMID]
2. Wright BE. The role of work context in work motivation: A public sector application of goal and social cognitive theories. J Public Adm Res Theory. 2004;14(1):59-78. [DOI]
3. Samadi Bilehsavar A, Nohesara S, Najarzadegan M, Molaei P, Alavi K, Nadoushan A. Investigation of Personality Traits in Attending of Iran University of Medical Sciences and Its Relation with General Health, Quality of Life and Job Burden. J Ardabil Univ Med Sci. 2017;17(1):90-103. [DOI]
4. Hamaideh SH. Occupational stress, social support, and quality of life among Jordanian mental health nurses. Issues Ment Health Nurs. 2012;33(1):15-23. [DOI] [PMID]
5. Pazokian M, Shaban M, Zakerimmoghadam M, Mehran A, Sanglaje B. The effect of stretching toghether aerobic exercise on fatigue level in multiple sclerosise patient reffer to MS society of Iran those suffer from fatigue. J Holist Nurs Midwifery. 2012;22(2):18-24. [Article]
6. Motamedzade M, Abbasinia M, Parvari R, Oliaie M, Karimi S, Mohammadi P. Mental workload and its association with fatigue in operating room personnel of Hamadan hospitals, Iran, 2016. J Occup Health Epidemiol. 2017;6(2):98-105. [DOI]
7. Sayady M, Omidi M, Bahrani MR, Reishahry AP. Evaluation and Comparing the Effectiveness of Meta- Cognitive and Progressive Muscle Relaxation Therapy for Chronic Fatigue of Bushehr City Nurses. Int J Manag Hum Sci. 2013;2(2):88-94.
8. Thomas EN, Blotman F. Aerobic Exercise in Fibromyalgia: A Practical Review. Rheumatol Int. 2010;30:1143-50. [DOI]
9. Bircan C, Karasel SA, Akgun B, El O, Alper S. Effects of Muscle Strengthening Versus Aerobic Exercise Program in Fibromyalgia. Rheumatol Int. 2008;28(6):527-32. [DOI] [PMID]
10. Johnston K, Carlyle L, Pattray S. Understanding MS and Exercise: A Fitness and Lifestyle Providers Guide. Alberta Division, Canada: MS Society of Canada; 2008. [Report]
11. Keogh JW, MacLeod RD. Body composition, physical fitness, functional performance, quality of life, and fatigue benefits of exercise for prostate cancer patients: a systematic review. J Pain Symptom Manage. 2012;43(1):96-110. [DOI] [PMID]
12. Aghajani MJ. The Professional Burnout of Nurses in different wards. J Res Dev Nurs Midwifery. 2013;9(2):97-104 [Article]
13. Buckle J. Clinical aromatherapy and AIDS. J Assoc Nurses AIDS Care. 2002;13(3):81-99. [DOI] [PMID]
14. Peng SM, Koo M, Yu ZR. Effects of music and essential oil inhalation on cardiac autonomic balance in healthy individuals. J Altern Complement Med. 2009;15(1):53-7. [DOI] [PMID]
15. Olapour A, Behaeen K, Akhondzadeh R, Soltani F, Al Sadat Razavi F, Bekhradi R. The effect of inhalation of aromatherapy blend containing lavender essential oil on cesarean postoperative pain. Anesth Pain Med. 2013;3(1):203-7. [DOI] [PMID] [PMCID]
16. Zadi Akhule O, Nasiri E, Lotfi M, Mahmoodi AA, Akbari H. The Effect of Concomitant Exercise and Inhalation of Lavender Fragrance on Surgical Technologists’ Fatigue Severity. J Health Saf Work. 2021;11(1):26-39. [Article]
17. Saremi M, Fallah MR. Subjective fatigue and medical errors among nurses in an educational hospital. Iran Occup Health. 2013;10(4):1-8. [Article]
18. Taha N, Azeaz M, Hassan A, Shaban A. Effect of Educational Program Regarding Therapeutic Exercises on Women’s Pain, Fatigue and Shoulder Function Undergoing Mastectomy. J Am Sci. 2013;9(3):412-25.
19. Arastoo AA, Ahmadi A, Zahednejad SH. The comparision of effect of 8 weeks aerobic and yoga training on physiological cost index in multiple sclerosis patients. Jundishapur Sci Med J. 2011;10(2):153-62.
20. Behbodi M, Atashzadeh Shorideh F, Nourian M, Jambarsang S, Mohtashami G .The Effect of Aerobic Exercise (Stretching Exercise) on The Fatigue Severity of Nurses in NICU. Nurs Midwifery J. 2015;12(12):1110-8. [Article]
21. Surakka J, Romberg A, Ruutiainen J, Aunola S, Virtanen A, Karppi SL, et al. Effects of aerobic and strength exercise on motor fatigue in men and women with multiple sclerosis: a randomized controlled trial. Clin Rehabil. 2004;18(7):737-46. [DOI] [PubMed]
22. Doring A, Pfueller CF, Paul F, Dorr J. Exercise in Multiple Sclerosis--an Integral Component of Disease Management. EPMA J. 2011;3(1):2. [DOI] [PMID] [PMCID]
23. Naji SA, Bahrani S, Mannani R, Bekhradi R. The effect of aromatherapy massage on fatigue in patients with multiple sclerosis. J Sabzevar Univ Med Sci. 2011;18(3):172-8. [URL]
24. Jo MJ. The effects of aroma inhalation on stress, fatigue, mood, and vital signs of the nurses in the operating rooms. J Korean Acad Adult Nurs. 2010;22(2):153-60.
25. Park SH, Park KS, Ko YJ, Lee BY, Yang HS, Park HJ, et al. The effect of aroma inhalation therapy on fatigue and sleep in nurse shift workers. J East West Nurs Res. 2012;18(2):66-73.
26. Bahrami T, Rejeh N, Heravi Karimooi M, Tadrisi SD, Amin G. Effect of Aromatherapy Massage on Fatigue and Hemodynamic Parameters in Elderly Women with Acute Coronary Syndrome. Nurs Midwifery J. 2016;14(4):343-51. [Article]
27. Sakamoto R, Minoura K, Usui A, Ishizuka Y, Kanba S. Effectiveness of aroma on work efficiency: lavender aroma during recesses prevents deterioration of work performance. Chem Senses. 2005;30(8):683-91. [DOI] [PMID]
28. Chnag SB, Chu SH, Kim YI, Yun SH. The effects of aroma inhalation on sleep and fatigue in night shift nurses. Korean J Adult Nurs. 2008;20(6):941-9.
29. Park H, Chun Y, Kwak S. The effects of aroma hand massage on fatigue and sleeping among hospice patients. Open J Nurs. 2016;6(7):515-23. [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution 4.0 International License. |
